
Manuscript accepted on :
Published online on: 07-01-2016
Plagiarism Check: Yes
Arif Yezdani1
Professor in Dept. of Orthodontics and Dentofacial Orthopaedics, Bharath University, Sree Balaji Dental College and Hospital, Narayanapuram, Pallikaranai,Chennai-600100
DOI : https://dx.doi.org/10.13005/bpj/698
Abstract
This case report highlights the treatment of a skeletal Class II malocclusion with pseudoanodontia that indicated clinical but not radiographic absence of teeth. A 21-year-old female patient presented with a skeletal Class II malocclusion with an orthognathic maxilla and a retrognathic mandible, with Angle’s Class I malocclusion with rotated maxillary and mandibular anteriors with fourteen impacted maxillary and mandibular teeth. Impacted mandibular right and left third molars were advised to be removed surgically. Maxillary right first premolar and left second premolar and mandibular right and left lateral incisors were surgically removed. Surgical exposure of the remaining multiple impacted teeth was done. Pre adjusted edgewise appliance, Roth’s prescription .018 inch slot was strapped up. Orthodontic extrusion of the impacted teeth was advocated. The seven impacted teeth were effectively treated with orthodontic traction. This improved the patients’ esthetics, speech and self-esteem considerably.
Keywords
multiple impacted teeth; surgical exposure; orthodontic traction
Download this article as:| Copy the following to cite this article: Yezdani A. Pseudoanodontia - Orthodontics To The Rescue?. Biomed Pharmacol J 2015;8(October Spl Edition) |
| Copy the following to cite this URL: Yezdani A. Pseudoanodontia - Orthodontics To The Rescue?. Biomed Pharmacol J 2015;8(October Spl Edition). Available from: http://biomedpharmajournal.org/?p=3655> |
Introduction
In clinical practice, delayed tooth eruption (DTE) is the most commonly encountered deviation from normal eruption time. It has been reported that DTE might be the primary or sole manifestation of local or systemic pathology.[1] Various genetic disorders and syndromes have DTE as a common feature.The delay in eruption was found to be greatest in children younger than 6 years but not much in those who were above 9 years.[2, 3] However, adults too have exhibited delayed tooth eruption. Individual, sexual, racial and ethnic factors can influence eruption and determine standards of normal eruption. [4, 5, 6] DTE can significantly impact the patient’s health care and can affect diagnosis, treatment planning and timing of treatment for the orthodontic patient.
Becker [7] suggested that root development alone should be the basis for defining the expected time of eruption for different teeth. Nonankylosed teeth too fail to erupt fully or partially because of malfunction of the eruption mechanism that occurs even though there seems to be no barrier to eruption and this phenomenon is considered to be due to a primary defect in the eruptive process.[8-10] Orthodontic traction of impacted teeth has been a standard and an accepted procedure in orthodontics.The following is a case report that attempts to use orthodontic traction to successfully erupt all the impacted teeth into the oral cavity.
Case Report
Diagnosis and etiology
A 21-year-old female patient presented with pseudoanodontia with crowded and rotated maxillary and mandibular incisors with speech difficulty.
Extraoral assessment. The patient had a mesoprosopic face, convex profile, posterior divergence, incompetent lips, with no signs of temporomandibular joint dysfunction.
Intraoral assessment. Oral hygiene was poor. The maxillary arch was U-shaped with crowded and rotated maxillary incisors with impacted 13, 15, 23, 24, and 25. The mandibular arch was V-shaped with severely rotated mandibular central incisors and impacted 32, 33, 38, 42, 43, 44, and 48. Retained 63 and severely carious16 with pronounced bulge in the alveolar mucosa in the upper right quadrant was observed. Increased overjet and deep bite was present. The maxillary and mandibular dental midlines coincided with each other and with the skeletal midlines. On left side the molar relation was Class I and the curve of Spee was increased. (Fig 1a-e, Fig 2a-b).
 |
Figure 1a: Pre-treatment intra-oral-Frontal |
 |
Figure 1b: Pre-treatment intra-oral-Right |
 |
Figure 1c: Pre-treatment intra-oral-Left |
 |
Figure 1d: Pre-treatment intra-oral-Upper Occlusal |
 |
Figure 1e: Pre-treatment intra-oral-Lower Occlusal |
 |
Figure 2a: Pre-treatment maxillary cast |
 |
Figure 2b: Pre-treatment mandibular cast |
Radiographic assessment. The panoramic radiograph confirmed the presence of impacted 13, 15, 23, 24, 25, 32, 33, 38, 42, 43, 44, and 48, with altered alveolar bone levels. (Fig 3).
 |
Figure 3: Pre-treatment panoramic radiograph |
Treatment objectives
The main treatment objective was to correct the pseudoanodontia and improve the speech and smile esthetics. Greater emphasis was laid for the correction of the crowded and rotated maxillary and mandibular incisors and to attempt orthodontic traction of the multiple impacted teeth.
Treatment alternatives
The severely impacted teeth could have been surgically removed and a prosthesis been given to replace the missing teeth, but the patient was not desirous of the same. The second alternative was to surgically expose the multiple impacted teeth and apply orthodontic traction to erupt these teeth. Patient was willing to undergo the second alternative to salvage the unerupted teeth.
Treatment progress
Deeply carious 16 and retained 63 were extracted. Pre adjusted edgewise appliance, Roth’s prescription .018 inch slot was strapped up prior to the surgical procedure. Flaps were raised in the maxillary and the mandibular dental arches and the severely rotated 14 which was an impediment for the orthodontic traction of 13 and 25 which was ectopically placed was surgically removed due to poor prognosis. 32 and 42 too were surgically removed. Subsequent to maintaining a moisture-less field in the vicinity of the impacted teeth, these teeth were bonded with their respective brackets with a dangling stainless steel ligature wire to assist in closed orthodontic traction. The flaps were subsequently closed back and sutured. After a week the sutures were removed and orthodontic traction was commenced with light force. (Fig 4). After successful orthodontic traction, leveling and alignment was done with 0.014 and 0.016 inch nickle titanium archwires. Space consolidation was done with 0.017 x 0.025 stainless steel archwires and final detailing and finishing with 0.019 x 0.025 stainless steel archwires.
 |
Figure 4: Surgical exposure and orthodontic traction |
Treatment outcome
The patient showed remarkable improvement in the correction of the multiple impacted teeth. 13, 15, 23, 24, 33, 34, and 43 were successfully erupted with orthodontic traction. After treatment, good facial harmony, balance and smile esthetics was achieved. Speech improved drastically. Normal overjet was achieved with alignment of maxillary and mandibular anteriors.The post treatment panoramic radiograph showed normal levels of alveolar bone with no root resorption (Fig 5). The post treatment lateral cephalometric radiograph was taken to gauge the treatment changes that was achieved. Endodontic treatment was done for 21 and 22 and fixed partial denture was given for 21, 22 .
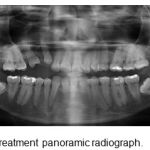 |
Figure 5: Post-treatment panoramic radiograph |
Discussion
Pseudoanodontia is a descriptive term that indicates clinical but not radiographic absence of teeth that should normally be present in the oral cavity for the patient’s dental and chronologic age. The cause could have been retained deciduous teeth or that the deciduous teeth had shed but the permanent ones had failed to erupt. Delayed tooth eruption is a condition where the tooth has developed more than the root length expected for eruption but remains unerupted. Gron11 showed that tooth eruption begins when ¾ of its final root length is established whereas normal biologic eruption time is defined as tooth eruption that occurs when the dental root is approximately 2/3 its final length. Rasmussen and Kotsaki [12] suggested using established norms for mean eruption ages calculated from population studies. By the norms suggested the case exhibited delayed tooth eruption despite the patient being 21 years of age. Various local conditions like supernumerary teeth [13], mucosal barrier [14], gingival hyperplasias [15], scar tissue [16], and tumors like odontomas [17] cause DTE. Traumatic injuries can lead to ectopic eruption or physical displacement of the permanent germ [18,19] or disruption in normal odontogenesis in the form of dilacerations.[20] Ankylosis and arch-length deficiency are also etiologic factors for crowding and impactions. [21] Systemic conditions like metabolic, endocrine and genetic disorders and drugs too can cause DTE. Extremes of nutritive deprivation on calcification and eruption have been reported.[22] A deficiency in an essential nutrient or a high metabolic demand on the growing tissues might influence the eruptive process. Endocrine disorders [23] like hypothyroidism, hypopituitarism, hypoparathyroidism, are associated with DTE. Renal failure [24] and anemic hypoxia [25] too have been correlated with DTE. The patient was anemic as gleaned by the blood reports. The delayed onset of the presence of a gene suggested for tooth eruption might be responsible for DTE in “inherited retarded eruption”.[12] This could explain the frequency of DTE in the posterior teeth which correlates with the case reported too. Lack of appropriate inflammatory response, increased bone density and inadequate expression of some cytokines that impede resorption have been noted to be factors for DTE in some syndromes.
The patient despite exhibiting fourteen impacted teeth did not have any supernumerary teeth or odontomas. The patient deferred the extraction of impacted 38 and 48 to a later date but was willing to undergo orthodontic traction for all the other seven impacted teeth. Orthodontic traction of impacted teeth has been widely reported in literature. [26, 27, 28] Orthodontic traction of the multiple impacted teeth was successfully performed alongwith established orthodontic bio-mechanics. No ankylosis was encountered during the process of orthodontic traction. 13, 15, 23, 24, 33, 34, and 43 were successfully erupted with orthodontic traction with light orthodontic force and the alveolar bone was well maintained due to this procedure. On the other hand, extraction of all the impacted teeth would have greatly compromised the alveolar bone level. 18 and 28 erupted normally as space was created in the maxillary arch during orthodontic treatment. Fixed prosthesis was given in 21, 22 region to enhance esthetics. The patient was insistent on removal of the appliance a little early than the prescribed time as she was getting married and hence effective extrusion of 13 and 15 could not be adequately achieved to provide for a fixed partial prosthesis for 13,14, and 15. The patients’ self-esteem, smile esthetics and speech improved dramatically.
Conclusion
Orthodontic traction of seven impacted teeth was successfully achieved in the case reported which in turn favourably improved the alveolar bone level and the patient was able to have a fairly good complement of teeth which undoubtedly improved her speech, mastication, occlusion and esthetics.
References
- Suri L, Gagari E, Vastardis H. Delayed tooth eruption: Pathogenesis , diagnosis, and treatment. A literature review. Am J Orthod Dentofacial Orthop 2004;126:432-45.
- Seow WK, Humphrys C, Mahanonda R, Tudehope DI. Dental eruption in low birth-weight prematurely born children: a controlled study. Pediatr Dent 1988;10: 39-42.
- Harila-Kaera V, Heikkinen T, Alvesalo L. The eruption of permanent incisors and first molars in prematurely born children. Eur J Orthod 2003;25: 293-9.
- Schour I, Massler M. The development of human dentition. J Am Dent Assoc 1941;28:1153-60.
- Nolla CM. The development of the human dentition. ASDC J Dent Child 1960;27:254-66.
- Moorrees CFA, Fanning EA, Hunt EEJ. Age variation of formation stages for ten permanent teeth. J Dent Res 1963;42:1490-502.
- Becker A. The orthodontic treatment of impacted teeth. London: Martin Dunitz; 1998.
- Proffit WR, Vig KW. Primary failure of eruption: a possible cause of posterior open bite. Am J Orthod 1981;80:173-90.
- O’Connell AC, Torske KR. Primary failure of tooth eruption: a unique case. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999;87:714-20.
- Pytlik W. Primary failure of eruption: a case report. Int Dent J 1991;41:274-8.
- Gron AM. Prediction of tooth emergence. J Dent Res 1962;41:573-85.
- Rasmussen P, Kotsaki A. Inherited retarded eruption in the permanent dentition. J Clin Pediatr Dent 1997;21;205-11.
- Shafer WG., Hine MK, Levy BM. Textbook of oral pathology. Philadelphia: W.B. Saunders;1983.
- Goho C. Delayed eruption due to overlying fibrous connective tissue. ASDC J Dent Child 1987;54:359-60.
- Katz J, Guelmann M, Barak S. Hereditary gingival fibromatosis with distinct dental, skeletal and developmental abnormalities. Pediatr Dent 2002;24:253-6.
- Di Biase DD. Mucous membrane and delayed eruption. Dent Pract Dent Rec 1971;21:241-50.
- Flaitz CM, Hicks J. Delayed tooth eruption associated with an ameloblastic fibro-odontoma. Pediatr Dent 2001;23:253-4.
- Hawe RR. Traumatized primary teeth. Dent Clin North Am 1966:391-404.
- Brin I, Ben-Bassat Y, Zilberman Y, Fuks A. Effect of trauma to the primary incisors on the alignment of their permanent successor s in Israelis. Community Dent Oral Epidemiol 1988;16:104-8.
- Andreasen JO, Andreasen FM. Textbook and colour atlas of traumatic injuries to the teeth. Copen hagen; Munksgaard;1994.
- Andreasen JO, Petersen JK, Laskin DM. Textbook and colour atlas of tooth impactions. St. Louis: Mosby;1997.
- Garn SM, Rohmann CG. Interaction of nutrition and genetics in the timing of growth. Pediatr Clin North Am 1966;13:353-79.
- Shaw L, Foster TD. Size and development of the dentition in endocrine deficiency. J Pedod 1989;13:155-60.
- Giglio MJ, Frid A, Barcat JA, Arrizurieta E. Depressed eruption dental rate in rats with hemodynamically mediated acute renal failure. Acta Odontol Lationoam 1994;8:27-37.
- Giglio MJ, Sanz AM, Bozzini CE. Depressed eruption rate of the rat maxillary incisor in a drug-induced uncompensated hemolytic state model. J Dent Res 1990;69:906-8.
- Richard Scott Conley, Scott B. Boyd. Harry L. Legan, Christopher C. Jernigan, Craig Starling and Christopher Potts. Treatment of patient with multiple impacted teeth. The Angle Orthodontist. 2007; 77:735-741.
- Chien-Lun Peng,Yu-Yu, Sheng-Yang Lee. Unilateral horizontally impacted maxillary canine and first premolar treated with a double archwire technique. The Angle Orthodontist 2006;76: 502-509.
- Giliana Clauser Zuccati, Tiziana Doldo. Multiple bilateral impactions in an adolescent girl. Am J Orthod Dentofacial Orthop 2010:137: S163-S172

