
Manuscript accepted on :
Published online on: 08-01-2016
Plagiarism Check: Yes
Vijay Ebenezer1, R. Balakrishnan2, Vigil Asir3, Swarna Priya4
1 Hod and Professor, Department of Oral and Maxillofacial Surgery , Sree Balaji Dental College and Hospital, Bharath University, Pallikaranai, chennai, 600100 2Professor, Department of Oral and Maxillofacial Surgery, Sree Balaji Dental College and Hospital, Bharath University, Pallikaranai, Chennai-600100 3Senior Lecturer, Department of Oral and Maxillofacial Surgery , Sree Balaji Dental College and Hospital, Bharath University, Pallikaranai, chennai, 600100 4Senior Lecturer, Department of Oral and Maxillofacial Surgery , Sree Balaji Dental College and Hospital, Bharath University, Pallikaranai, chennai, 600100
DOI : https://dx.doi.org/10.13005/bpj/709
Abstract
Dental implants were initiated in 1922 by Branemark, who and associates described the relationship between titanium implant and bone which termed osteointegration, defined as the direct structural and functional connection between living bone and the surface of an implant1 .This clinical review is to evaluate of the effectiveness of implants placed in severly atrophic mandible.
Keywords
Atrophic Maxilla; Mandible; Implants; Osseointegration
Download this article as:| Copy the following to cite this article: Ebenezer V, Balakrishnan R, Asir V, Priya S. A Case Report - Implant Placement In Resorbed Alveolus. Biomed Pharmacol J 2015;8(October Spl Edition) |
| Copy the following to cite this URL: Ebenezer V, Balakrishnan R, Asir V, Priya S. A Case Report - Implant Placement In Resorbed Alveolus. Biomed Pharmacol J 2015;8(October Spl Edition). Available from: http://biomedpharmajournal.org/?p=3716> |
Introduction
Bone loss that takes place in the edentulous alveolar ridge over time often impedes the use of standard implant placement protocols, and calls for alternative or additional procedures2. This case report supports the theory of increased patient acceptance of the rehabilitation procedure by using graftless solutions or nonautogenous sources of graft material. In cases of mild to moderate resorption, shorter and narrower implants3-5 as well as angled implant placement 6-9 may be effective strategies to avoid bone grafting are usually followed, in this case bone augmentation or split ridge was not used rather, sequential osteotome with drill bits of required size was done ,with care not to cause fracture to the mandible.
Case Report
A 77 yr old female patient reported with a chief complaint of pain on her temperomandibular joint for past eight months . History reveals that pt is a denture wearer for past 29 years . Her Last dentures were fabricated 11 yrs back. Patient complaints of floating denture in relation to mandible . On intra oral clinical examination , the ridge exhibited knife -edge ridge in maxilla and mandible and increased vertical dimensions. Patient was advised OPG (fig 1) which revealed severe atrophic edentulous maxilla and mandible ,this case was considered to be “complex” both in terms of the surgical and restorative aspects. On routine examination, pt was did not have any systemic disorders , patients blood pressure was 130/90mmhg. treatment planning was done . Since the patient had problem with the mandible , implant retained prosthesis was planned, patient was informed in detail about the procedure and informed consent was taken. routine blood investigations were done . Under local anesthesia , dental implants were placed in relation to 34 and 44 region in between the mental foramina. Care was taken not to fracture the mandible since its severely atrophic. primary stability was achieved, cover screw were placed. After six months OPG was taken (fig 2) , radiograph revealed no abnormality . Ball abutments was placed and denture retained prosthesis was given. Patient had regular follow up , with which patient did not have any complaints in occlusion nor in pain of temperomandibular joint
 |
Figure 1: Pre Operative Opg |
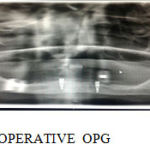 |
Figure 2: Post Operative Opg |
Discussion
Autogenous bone remains the “Gold Standard” for grafting. The autogenous graft may be harvested from many intra-oral sites. The maxillary tuberosity, anterior nasal spine, and zygomatic buttress have been reported for the upper jaw10,11,12. The mandibular symphysis, ascending ramus, coronoid process, and horizontal ramus are useful sites from the lower jaw 13 , but autogenous bone grafts needs patient consent and some do not accept harvesting bone from the donor site ,in this case elderly patient did not accept for any augmentation , following this there are more chances of secondary infection following the grafts and non healing of donor site. Thus implants were placed without an grafts , through which fair prognosis of the implant was achieved. In this case of severe atrophy of the maxilla and mandible , the implant was placed in the mandible without any Alveolar ridge reconstruction or Spilt ridge bone augmentation. thus consuming less time and providing accepted results in elderly patients.
Standard Implant placement protocol with suitable individual modification according to bon quality in surgeons hand can obviate the need for extended surgical procedure.
Reference
- Albrektsson T, Branemark P, Hansson H & Lindstrom J. (1981). Osteointegration titanium implants. Acta Orthop Scand 52: 155-159
- Araujo MG, Sonohara M, Hayacibara R, Cardaropoli G, Lindhe J. Lateral ridge augmentation by the use of grafts comprised of autologous bone or a biomaterial. An experiment in the dog. J Clin Periodontol 2002;29:1122–1131.
- Arisan V, Bolukbasi N, Ersanli S, Ozdemir T. Evaluation of 316 narrowdiameter implants followed for 5-10 years: A clinical and radiographic retrospective study. Clin Oral Implants Res 2010;21:296–307.
- Menchero-Cantalejo E, Barona-Dorado C, Cantero-Alvarez M,Fernandez-Caliz F, Martinez-Gonzalez JM. Meta-analysis on the survival of short implants. Med Oral Patol Oral Cir Bucal 2011;16: e546–551.
- Neldam CA, Pinholt EM. State of the art of short dental implants:A systematic review of the literature. Clin Implant Dent Relat Res 2010 Oct 26 [epub ahead of print].
- Aparicio C, Perales P, Rangert B. Tilted implants as an alternative to maxillary sinus grafting : A clinical, radiologic, and periotest study. Clin Implant Dent Relat Res 2001;3:39–49.
- Krekmanov L, Kahn M, Rangert B, Lindstrom H. Tilting of posterior mandibular and maxillary implants for improved prosthesis support. Int J Oral Maxillofac Implants 2000;15:405–414.
- ten Bruggenkate CM, Sutter F, Oosterbeek HS, Schroeder A. Indications for angled implants. J Prosthet Dent 1992;67:85–93.
- Testori T, Del Fabbro M, Capelli M, et al. Immediate occlusal loading and tilted implants for the rehabilitation of the atrophic edentulous maxilla: 1-year interim results of a multicenter prospective study. Clin Oral Implants Res 2008;19:227–232.
- Tolstunov, L. Maxillary Tuberosity Block Bone Graft: Innovative Technique and Case Report. J Oral Maxillofac Surg 2009; 67:1723- 1729.
- Buser,D. “State of the Art Surgical Procedures in Esthetic Implant Dentistry.” Straumann training Lecture. Hong Kong. October 6,2009.
- Gellrich,N. et al. Alveolar Zygomatic Buttress: A New Donor Site for Limited Preimplant Augmentation Procedures. J Oral Maxillofac Surg 2007; 65:275-280.
- Soehardi,G. et al. The Potential of the Horizontal Ramus of the Mandible as a Donor Site for Block and Particular Grafts in Preimplant Surgery. Int J Oral Maxillofac Surg 2009; 38:1172-1178

