
Manuscript accepted on :
Published online on: --
Plagiarism Check: Yes
Ghasem Dastjerdi1, Hamid Mirhoseini2 and Ehsan Mohammadi3
1Assistant Professor of Psychiatry, Yazd Shahid Sadooghi University of Medical Sciences, Yazd, Iran. 2PhD Candidate in Neurosciences, Yazd Shahid Sadooghi University of Medical Sciences, Yazd, Iran. 3Residents of Psychiatry, Faculty of Medicine, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran.
DOI : https://dx.doi.org/10.13005/bpj/885
Abstract
Despite recent advances in antidepressant medication as the main treatment option for severe depression, large portion of patients are drug resistant. The side effects of the drugs sometimes occur before the treatment effects which can terminate the treatment process. Therefore, developing new efficient and safe alternative treatment is the main focus of scientific societies. The present study aimed to comparatively investigate the synergistic therapeutic effects of transcranial direct current stimulation (tDCS) and cranial electrical stimulation (CES) in major depression in a double blinded randomized controlled trial. This was a double blinded randomized controlled trial conducted on 30 major depression patients diagnosed by semi-structured review of DSMiv-TR by a psychologist. The patients filled the Beck Depression Inventory (BDI-II) and Beck Anxiety Inventory (BAI). The quantitative electroencephalograms of patients were recorded and analyzed with Neuroguide processing tool to determine the regions with abnormal function using the age and gender matched standard databases of quantitative electroencephalogram (QEEG0. Thirty patients were randomly divided into three groups: CES, combined CES-tDCS, and CES treatment. Each patient receive 6 sessions consisting of 3 consequtive days and 3 sessions on the every other day basis (3 sessions a week) of 20-min exposure. After the 6 treatment sessions the patients were asked to fill the BDI-II and BAI questionnaires. The combined treatment showed more response followed by CES and tDCS treatments (P<0.01). In addition, no significant difference was observed in the treatments’ complications between the three groups (P>0.01). However, disease duration was significantly different between the three groups (P<0.01). Our findings showed that QEEG guided treatment with tDCS and CES can be effective in depression. It seems that tDCS acts through regulating the firing rate of cortical neurons and CEW through modulating the thalamus and limbic system in treatment of depression. Combined CES-tDCS can yield more efficient treatment.
Keywords
Cranial electrical Stimulation; Beck Depression Inventory; Beck Anxiety Inventory; Depression Treatment; transcranial Direct Current Stimulation; Combined treatment
Download this article as:| Copy the following to cite this article: Dastjerdi G, Mirhoseini H, Mohammadi E. Investigating the Synergistic Effects of Transcranial Direct Current Stimulation and Cranial Electrical Stimulation in Treatment of Major Depression in A Double Blinded Controlled Trial. Biomed Pharmacol J 2015;8(2) |
| Copy the following to cite this URL: Dastjerdi G, Mirhoseini H, Mohammadi E. Investigating the Synergistic Effects of Transcranial Direct Current Stimulation and Cranial Electrical Stimulation in Treatment of Major Depression in A Double Blinded Controlled Trial. Biomed Pharmacol J 2015;8(2). Available from: http://biomedpharmajournal.org/?p=6193 |
Introduction
Depression is one of the most common disorders worldwide and more than 350 million people suffer from various types of this disease [1]. Its symptoms include fatigue, sleeplessness, suicidal thoughts, suicide attempts, digestive problems, frustration, isolation, lack of concentration, memory loss, etc[2, 3]. In addition to these symptoms,brain imaging techniques show that different regions of the brain undergo significant physiological and functional changes[4-6]. In addition to the personal and social aspects of human life, depression’s symptoms adversely influenceseveral physiological and psychological functions of the patient which make the treatment of depressive disorders as one of the world’s most expensive medical treatment [1, 7-9].American Psychiatric Association recognizes four main groups of treatments for depression which are drug therapy, psychotherapy, drug therapy plus psychotherapy, and electroconvulsive therapy (ECT) [7, 10]. Despite using of different antidepressants drugs, some portion of depressed patients are resistant to drug treatment [11]. Therefore, developing nonpharmacologic is necessary for depression treatment.
During the recent years, physical agents such as electrical and magnetic fields, sound waves and laser have been extensively used as alternative or adjunctive treatments for different disorders ranging from musculoskeletal, metabolic disorders, wounds, and neuropsychiatric disorders[12-17].Despite recent advances in antidepressant medication as the main treatment option for severe depression, large portion of patients are drug resistant. The side effects of the drugs sometimes occur before the treatment effects which can terminate the treatment process. Therefore, developing new efficient and safe alternative treatment is the main focus of scientific societies. The present study aimed to comparatively investigate the synergistic therapeutic effects of transcranial direct current stimulation (tDCS) and cranial electrical stimulation (CES) in major depression in a double blinded randomized controlled trial.
Materials and Methods
This study is a randomized double-blind clinical trial. The study population consisted of 30 patients (three n=10 groups) of between 18 and 55 years, who have been diagnosed by psychiatrists to have major depressive disorder based on the text revision of the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV). Having accepted and signed the written consent form, the patients with depressive disorder based on DSM-IV criteria were selected using the table of random numbers cooperated by a statistics consultant and were studied in three n=10 groups, GroupA with tDCSOn and CES offas sham, Group B with both tDCSand CESOn (combined tDCS-CES), and Group Cwith CES On andTDCS off as sham. The devices were used separately and the excitement time was 20 minutes for each session. As the patients arrived, they were asked to fill 21-item Beck Depression Inventory (BDI) and 21-item Beck Anxiety Inventory (BAI). Electroencephalogram (EEG) and Quantitative Electroencephalogram (QEEG) were then used for the patients, and they were finally reassessed using Beck Anxiety Questionnaire and Depression Inventory, and the changes occurring usingthese scales were assessed. All of the patients were treated first within three successive days and then every other day (three sessions per week) for ten days in 6 twenty-minute sessions (for each device in each method). At the beginning of the sessions, the patients were tested using electrophysiological QEEG mapping and due to the primary electrophysiological disorders of electrodes, the devices were then installed in specific places in order to normalize the disrupted waves.At the end of the sixth session, the patients were assessed using BDI and BAI scales. After the data were collected, they were entered into SPSS 20 Software and were then analyzed using Chi-square Test, Paired T-test and Analysis of Variance (ANOVA) Test.
Results
On the whole, 30 patients who were just treated using tDCS, CES, and combinedtDCS-CES, and who had the required criteria were selected as the sample. The patients were divided into three n=10 groups, namely Group A, Group B and Group C. The patients of Group Awere studied with CES on and tDCSoff as (Sham), those of Group B were studied with tDCSon and CES off as (Sham) and Group three using both tDCSand CES on. The frequency distribution of the patients’ gender and average age in three therapy groups ispresented in Tables 1 and 2.
Table 1: The frequency distribution of the patients’ gender in the three groups under study
| total | male | female | Group |
| 10 (100%) | 4 (40%) | 6 (60%) | Group A |
| 10 (100%) | 4 (40%) | 6 (60%) | Group B |
| 10 (100%) | 5 (50%) | 5 (50%) | Group C |
| 30 (100%) | 13 (43.3%) | 17 (56.7%) | total |
Based on the Table 1, the Chi-square Test and the P-value (0.33), it can be concluded thatgender had no significant difference among the three intervention groups.
Table 2: A comparison of the patients’ age average in the three groups
| number | Mean ±Standard deviation (years) | variable |
| 10 | 7.09± 30.1 | Group A |
| 10 | 7.17 ± 34.1 | Group B |
| 10 | 10.83 ± 30.2 | Group C |
Based on the table above, the T-test and the P-value (0.86), it can be concluded thatage had no significant difference among the three intervention groups. A comparison of the treatment complicationsin the three groups under study is presented in Table 3.
Table 3: Frequency of the treatment complications among the three intervention groups
| percentage | frequency | group |
| 10% | 1 | Group A |
| 0% | 0 | Group B |
| 10% | 1 | Group C |
Based on the table above, the Chi-square Test and the P-value (0.83), it can be concluded that treatment complications have had no significant difference among the three intervention groups.
The disease duration in the three groups is compared and presented in Table 4.
Table 4: Disease duration frequency among the three groups
| > 5 years | 2-5 years | <2 years | group |
| 0 | 3 | 7 | Group A |
| 0 | 2 | 8 | Group B |
| 0 | 3 | 7 | Group C |
Based on the Table 4, the T-test and the P-value < 0.1, it can be concluded thatdisease duration has had no significant difference among the three intervention groups.
The three groups of patients were examined and compared before and after the test in terms of anxiety and depression rate (Tables 5 & 6).
Table 5: Results of comparing the three groups in termsof depression and anxiety (before the test)
| significance | Group C | Group B | Group A | |
| 0.47 | 7.6±26.2 | 6.1±28.2 | 6.7±25.7 | depression |
| 0.02 | 5.2 ±18.4 | 5.84 ±15.00 | 6.6 ±14.1 | anxiety |
Based on the table above, the T-test and the P-value (0.47), it can be concluded thatthe depression test score has had no significant difference among the three intervention groups before the intervention, while there was a significant difference among them in terms of anxiety.
Table 6: Results of comparing the three groups in terms of depression and anxiety (after the test)
| significance | Group C | Group B | Group A | |
| 0.003 | 1.5 ± 8.90 | 4.93 ± 16.70 | 6.6± 10.00 | depression |
| 0.05 | 3.1 ± 7.0 | 5.3± 09.90 | 5.1± 2.2 | anxiety |
Based on the Table 6, the ANOVA Test and the P-Value<0.001, it can be concluded thatthe depression test score has had a significant difference among the three intervention groups after the intervention. As presented in Table 5, the difference among the groups in terms of anxiety after administration of the test has also been significant.
The three groups’ scores of depression and anxiety before and after the intervention werecompared with and the results are shown in Figures 1 and 2.
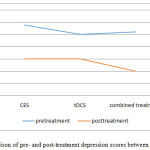 |
Figure 1: A comparison of pre- and post-treatment depression scores between the three groups |
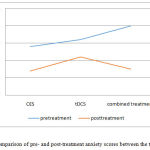 |
Figure 2: A comparison of pre- and post-treatment anxiety scores between the three groups |
Discussion and Conclusion
We studied and compared the effect of tDCS, CES, and combined tDCS-CES in treating major depression. It was shown in this study that there was a significant difference among the patients who were placed in three different groups to be treated differently (Table 6). It was also shown that Group C, which had used the two therapies showed less rate of depression and anxiety than the other two groups that had used either tDCS or CES. The CES method was also shown to be more effective for treatment of depression and anxiety than the tDCS method. Due to the great effect of tDCS on depression and its reduction of negative feelings and enhancement of positive feelings, it can be concluded thatt DCS adjusts the cerebral cortex waves which had been taken based on primary QEFG and patients’ age. This result was in line with another research which showed that TDCS can affect the general arousal level and raise attention to the frontal lobe of the brain.
Depression causes a change or disorder in the balance and dynamics of the left hemisphere of the brain, and causes the two hemispheres of the brain to act differently in cognitive and emotional processes. However, tDCScan induce a balance between the two hemispheres and helps improve the depressive disorder in this way [18]. As different areas of the brain were recognized in this research and tDCS was placed in the hyperactive and inactive areas of the brain, it was shown that detecting the damaged area of the brain is very effective in the therapy process. This finding is in line with another study indicating that tDCSexerted its physiological effects within a few minutes to hours on the dorsolateral prefrontal cortex (Anode: right, cathode: left) the left hemisphere to the right hemisphere and thus affectedthe moods and reduced the depression and anxiety rate in the subjects. What attracted our attention was that the depression rate was also affected by the places of electrodes as well as by their diameter and stream. [19].
Another reason is that tDCS adjusts the neuronal firing of different parts of cortex and this causes the cortex of the brain to adjust the neurons and thus affect the patient’s mood and behavior. Another research also showed that tDCS causes long-term synapses, which in turn cause the neurotropic activity of the brain. The research showed that the type and degree of brain injury and the time when the illness starts also affect the therapy [20]. Another research showed that TDCS creates changes in the frontal lobe and the left frontal skull and thus creates antidepressant properties [21].
The mechanism of CES influence can also be explained in the following way: CES adjusts the blood flow between the two hemispheres of the brain and thus adjusts the limbic system, the thalamus, and the basal ganglia. Different studies have shown that CES has considerably helped CSF(cerebrospinal fluid) andplasmaserotonintreatment-resistantdepression [22]. Therefore, the basal ganglia and the thalamus help reduce the depression rate by adjusting the serotonin [23].
Another research also showed that CES influences the brain system by changing the level of hormones and neurotransmitters [24]. Another report about the clinical improvement in depression and anxiety showed that CES enhancesmonoamine oxidaseactivityandplasmaconcentration from Gamma-amino butyric acid [25]. Moreover, CES increases the levels of catecholamine in both males and females and increases the production of thyroxin in those males who receive CES for a long period of time [26]. A research which studied the changes of EEG showed that CES reduces the beta wave power and modifying the abnormality of these two waves helps create therapeutic effects [25].
The results of several studies show that CES influences different regions of the brain compared with the tDCS.
The influence of CES has been reported by different studies to be between 30 and 40 percent [26, 27], while that of tDCS has been shown to be between 35 and 40 percent [29, 18]. It was shown in this research that as the two methods have no serious and dangerous complications and the selection of patients was in such a way that it reduced the possibility of complications, and also because no researchhas argued against this combination, the two methods were combined in this research. This combination increased their effect up to 66 percent due to the simultaneous stimulation of different areas of the brain, which affects one’s mood and behavior.
Considering what has been mentioned so far, we can come to the conclusion that the integration of the two therapies will help improve depression due to the effect of tDCS on cortex and that of CES on the limbic and the thalamus, which are parts of the brain that adjust one’s mood.
Since depression paves the way for anxiety in an individual, it is expected that the reduction of depression will lead to the reduction of anxiety in the patient, which actually happened in the present research. About 85% of the patients with depressive disorder experience considerable symptoms of anxiety, and similarly, 90% of the patients with anxiety disorders become depressed too [30]. Anxiety was not followed as a main factor in the present research, but it was investigated as a peripheral factor. However, it was shown that the reduction of the patients’ depression resulted in the significant reduction of their anxiety. It can thus be concluded that the CES and tDCS therapies are very effective in managing depression and anxiety.
It was shown in Table (4), related to the second hypothesis, that the mean score of depression with three methods of CES, tDCS, and both tDCSand CES has not been significant in terms of disease duration. The result of this research is in line with the conclusions made by Nilsson et al., and Bernini et al. The result of this research can be justified in that the depression duration among the sample subjects has been nearly similar, or the difference has not been significant. However, other studies have shown that the reason for the insignificant difference in terms of disease duration is due to the small number of the sample size. No definite conclusion can be made from this hypothesis and more extensive studies are actually needed for it.
In testing the third hypothesis, a comparison of the frequency distribution of the treatment complications using the three methods of CES, tDCS and both tDCSand CES showed no significant effect after the intervention. It is noteworthy that only two cases of headache were observed among the 30 subjects of the research, one in the group that had used the tDCS method and the other in the combination therapy group (Group C). The research results are in line with the research conducted by Nietzsche [36]. Similar studies have also shown that tDCS has had a few complications such as headache [32, 33, 34, 37, 39], but the studies have provided no reason for this problem. However, another research showed skin complications with greater erythema and browning of the skin [38]. However, the present research has showed no symptoms of erythema or browning of the skin, because the stimulation in this research was less than 2 mA and gel or pad soaked in a solution of salt was used and the stimulation was done twice a week. The stimulation in the research that was mentioned earlier [38] was, however, 2-3 mA and tDCS stimulation was done five times a week.
References
- Lépine, J.-P. and M. Briley, The increasing burden of depression. Neuropsychiatric disease and treatment, 2011. 7(Suppl 1): p. 3.
- Lépine, J.-P., Epidemiology, burden, and disability in depression and anxiety. The Journal of clinical psychiatry, 2000. 62: 4-10; discussion 11-2.
- Marcus, M., et al., Depression: A global public health concern. Retrieved February, 2012. 7: p. 2014.
- Anderson, J.E., et al., An MRI study of temporal lobe abnormalities and negative symptoms in chronic schizophrenia.Schizophrenia research, 2002. 58(2): p. 123-134.
- Kwon, J.S., T. Youn, and H.Y. Jung, Right hemisphere abnormalities in major depression: quantitative electroencephalographic findings before and after treatment. Journal of affective disorders, 1996. 40(3): 169-173.
- Koolschijn, P., et al., Brain volume abnormalities in major depressive disorder: A meta‐analysis of magnetic resonance imaging studies. Human brain mapping, 2009. 30(11): p. 3719-3735.
- Ali, Y. and N.A. Mahmud, Neurofeedback treatments for depression disorders: review of current advances. J. Comp. Sci. & Technol., 2014. 7(3): p. 443-452.
- Health, N.C.C.f.M. Depression: the treatment and management of depression in adults (updated edition). 2010. British Psychological Society.
- Von Korff, M., et al., Treatment costs, cost offset, and cost-effectiveness of collaborative management of depression. Psychosomatic medicine, 1998. 60(2): p. 143-149.
- Association, A.P. and A.P.A.W.G.o.B.P. Disorder, Practice guideline for the treatment of patients with borderline personality disorder. 2001: American Psychiatric Pub.
- Fava, M. and K.G. Davidson, Definition and epidemiology of treatment-resistant depression. Psychiatr Clin North Am, 1996. 19(2): p. 179-200.
- Mostafa, J., etal., Electromagnetic Fields and Ultrasound Waves in Wound Treatment: A Comparative Review of Therapeutic Outcomes., Biotech. Res. Asia, 2015. 12(Spl.Edn.1): p. 185-195.
- Yadollahpour, A. and S. Rashidi, A Review of Electromagnetic Field BasedTreatments for Different Bone Fractures., Biotech. Res. Asia, 2014. 11(2): p. 611-620.
- Yadollahpour, A. and S. Rashidi, Therapeutic Applications of Electromagnetic Fields in Musculoskeletal Disorders: A Review of Current Techniques and Mechanisms of Action. Biomedical and Pharmacology Journal, 2014. 7(1): p. 23-32.
- Yadollahpour, A., S. Rashidi, and Z. Ghotbeddin, Electromagnetic Fields for the Treatments of Wastewater: A Review of Applications and Future Opportunities. J Pure Appl Microbio, 2014. 8(5): 3711-3719.
- Yadollahpour, A. and Z. Rezaee, Electroporation as a New Cancer Treatment Technique: A Review on the Mechanisms of Action. Biomedical and Pharmacology Journal, 2014. 7(1): p. 53-62.
- ZOHRE, R., et al., Nondrug Antimicrobial Techniques: Electromagnetic Fields and Photodynamic Therapy. Biomedical and Pharmacology Journal, 2015. 8(March Spl Edition): p. 147-155.
- Cattaneo Z, Pisoni A, Papagno C. Transcranial direct current stimulation over Broca’s region improves phonemic and semantic fluency in healthy individuals. Neuroscience. 2011 Jun 2; 183:64-70. PubMed PMID: 21477637.
- Koenigs M, Ukueberuwa D, Campion P, Grafman J, Wassermann E. Bilateral frontal transcranial direct current stimulation: Failure to replicate classic findings in healthy subjects. Clinical neurophysiology: official journal of the International Federation of Clinical Neurophysiology. 2009 Jan; 120 (1):80-4. PubMed PMID: 19027357. Pubmed Central PMCID: 2650218.
- Volpato C, Cavinato M, Piccione F, Garzon M, Meneghello F, Birbaumer N. Transcranial direct current stimulation (tDCS) of Broca’s area in chronic aphasia: a controlled outcome study. Behavioural brain research. 2013 Jun 15; 247:211-6. PubMed PMID: 23538068.
- Galvez V, Alonzo A, Martin D, Mitchell PB, Sachdev P, Loo CK. Hypomania induction in a patient with bipolar II disorder by transcranial direct current stimulation (tDCS). The journal of ECT. 2011 Sep; 27(3):256-8. PubMed PMID: 21206371.
- Shealy CN. Transcutaneous electrical nerve stimulation: the treatment of choice for pain and depression. J Altern Complement Med. 2003. 9: 619-623.
- Schroeder M, Barr R. Quantitative analysis of the electroencephalogram during cranial electrotherapy stimulation. Clinical Neurophysiology. 2001; 112(11):2075-83.
- Ferdjallah M, Bostick FX Jr, Barr RE. Potential and current density distributions of cranial electrotherapy stimulation (CES) in a four-concentricspheres model. IEEE Trans Biomed Eng. 1996. 43: 939-943.
- Jarzembski WB. Electrical stimulation and substance abuse treatment. NeurobehavToxicolTeratol. 1985. 7: 119-123.
- Antal A, Terney D, Kuhnl S, Paulus W. Anodal transcranial direct current stimulation of the motor cortex ameliorates chronic pain and reduces short intracortical inhibition. Journal of pain and symptom management. 2010 May;39(5):890-903. PubMed PMID: 20471549.
- Feusner JD, Madsen S, Moody TD, Bohon C, Hembacher E, Bookheimer SY, et al. Effects of cranial electrotherapy stimulation on resting state brain activity. Brain and behavior. 2012 May;2 (3):211-20. PubMed PMID: 22741094. Pubmed Central PMCID: 3381625.
- Kirsch DL, Nichols F. Cranial electrotherapy stimulation for treatment of anxiety, depression, and insomnia. The Psychiatric clinics of North America. 2013 Mar; 36 (1):169-76. PubMed PMID: 23538086.
- Alexander T, Avirame K, Lavidor M. Improving emotional prosody detection in the attending ear by cathodaltDCS suppression of the competing channel. Neuroscience letters. 2012 Feb 2; 508(1):52-5. PubMed PMID: 22206843.
- Gorman JM. Comorbid depression and anxiety spectrum disorders. Depression and anxiety. 1996;4(4):160-8. PubMed PMID: 9166648.
- Brunoni AR, Ferrucci R, Bortolomasi M, Vergari M, Tadini L, Boggio PS, et al. Transcranial direct current stimulation (tDCS) in unipolar vs. bipolar depressive disorder. Progress in neuro-psychopharmacology & biological psychiatry. 2011 Jan 15;35(1):96-101. PubMed PMID: 20854868.
- Jonathan Walker. Robert Lawson, Gerald Kozlowski. Current Status of QEEG and Neurofeedback in the Treatment of Clinical Depression. A Neurotherapy Center of Dallas and University of Texas Southwestern Medical School, Dallas. Edited by James R. Evans.
- FregniF,BoggioPS,NitscheMA, et al.Treatmentofmajordepressionwithtranscranial direct current stimulation. Bipolar Disord 2006;8:203-205.
- Boggio PS, Rigonatti SP, Ribeiro RB, et al. A randomized, double-blind clinical trail on the efficacy of cortical direct current stimulation for the treatment of major depression. Int J Neuropsychopharmacol 2008;11: 249-254.
- Rigonatti SP, Boggio PS, Myczkowski ML, et al. Transcranial direct stimulation and fluoxetine for the treatment of depression. Eur Psychiatry 2008;23:74-76.
- Nitsche MA, Liebetanz D, Lang N, et al. Safety criteria for transcranial direct current stimulation (tDCS) in humans. ClinNeurophysiol 2003; 114:2220-2222.
- Iyer MB, Mattu U, Grafman J, et al. Safety and cognitive effect of frontal DC brain polarization in healthy individuals. Neurol 2005; 64:872-875.
- Blumberger, D.M., Tran, L.C., Fitzgerald, P.B., Hoy, K.E., Daskalakis, Z.J.,. A randomized double-blind sham-controlled study of transcranial direct current stimulation for treatment-resistant major depression. Front. Psychiatry 2012. 3, 74.
- Palm U, Keeser D, Schiller C, Fintescu Z, Nitsche M, Reisinger E, et al. Skin lesions after treatment with transcranial direct current stimulation (tDCS). Brain stimulation. 2008 Oct;1(4):386-7. PubMed PMID: 20633396.

