
Manuscript accepted on :
Published online on: 08-01-2016
Plagiarism Check: Yes
Vahid Fakhrzadeh1, Tahere Gaffari1, Fahimeh Hamedirad1, Ramin Negahdari1, Alireza Pour Nasrollah1 and Hosein Eslami2*
1Department of Prosthodontic Dentistry, Faculty of Dentistry, Tabriz University of Medical Sciences, Tabriz, Iran 2Department of Oral Medicine Dentistry, Faculty of Dentistry, Tabriz University of Medical Sciences, Tabriz, Iran
DOI : https://dx.doi.org/10.13005/bpj/823
Abstract
The use of porcelain laminate due to increasing patient demand for aesthetic restorations frequently and their application to deal with badly formed teeth reconstruction has been one of the most important criteria for clinical evaluation of fixed restoration, compliance margin. Purpose of this study was to evaluate two different marginal in two different cutting porcelain laminate veneer, is to make two dental acrylic labial surface of the maxillary incise edges to two common ways of cutting laminate (CNC). Cutting 2-mm edge along was done with the expansion of the lingual incisal chamfer form and was shaved and molded build two master metal die after each group of 30 that included 15 veneers felt spastic veneer laminate veneer Duce ram and 15 are made of core Interim. Results indicated significant differences based on the type of prepared cutting gap observed in various areas cutting rate between gap showed significant difference(P <0.01) also, the rate gap based on the type of laminate is a significant differences (P<0.05). .In cream laminate veneers in the marginal rate mismatch in the clinical range are acceptable but Duce ram laminate veneers is not acceptable.
Keywords
porcelain laminate; increasing patient; acceptable; Influence of Preparation
Download this article as:| Copy the following to cite this article: Fakhrzadeh V, Gaffari T, Hamedirad F, Negahdari R, Nasrollah A. P , Eslami H . Influence of Preparation Design and Restorative Material to Marginal Discrepancy of Ceramic Laminate Veneers. Biomed Pharmacol J 2015;8(2) |
| Copy the following to cite this URL: Fakhrzadeh V, Gaffari T, Hamedirad F, Negahdari R, Nasrollah A. P , Eslami H . Influence of Preparation Design and Restorative Material to Marginal Discrepancy of Ceramic Laminate Veneers. Biomed Pharmacol J 2015;8(2). Available from: http://biomedpharmajournal.org/?p=3731 |
Introduction
Over the past decade, the use of porcelain laminate due to increasing patient demand for aesthetic restorations frequently and their application has been successful for the reconstruction deal with badly formed teeth. (1). Durable ceramic veneers clinically after 15 years at a rate of 93% has been reported that this success by taking factors such as the preservation of tooth structure, enamel quality connection to the beauty and the stability of the color (2,3) The beauty of all-ceramic crowns demand have led to the restoration of the most popular, become. This restoration of strength and success is marginal as the two main factors (4). One of the important criteria for clinical evaluation of fixed restorations is marginal adaptation (5). Mismatch studied various restoration and study, have reported mixed results. But most of the clinically acceptable value is 100 mm (6). Christensen reported that the degree of mismatch between the gingival margin below the gingival margin between 119-34 mm and 51-2 mm (7). Mclean announced that 120 microns, maximum marginal gap is accepted at the clinic (8-10). Tuntiprawon and Wilson showed that ceramic crown with values smaller Gap Axial and marginal on the die wall, had the highest compressive strength (11). Type of preparation is one of the main controversial about this type of restoration are generally four types of preparation for the veneer have been proposed preparation Window limited to labial surface of the tooth is the preparation Feathered incisal edge (extending to Marzyn incisal but without specifying Finish line).(2) The fundamental problem of feldspathic porcelain, alumina ceramic restorations are low flexural strength (Mpa 200-75) (13) and Fracture toughnes (MP5/2-5/1) and defeated a force of occlusal forces in the anterior teeth (N 200-60) and the posterior occlusal force than the mouth (N 450-200) is (14,15). 4). A number of researchers from several distinct points, with a small distance from each other, which is 150-18 points around a recap / abutment was used to assess (29, 22).
Methods
The labial surface of the maxillary acrylic teeth (AB-3; Fraco, Tettang, Germany) was used before cutting (to equal the thickness of the veneer in all samples) and Poti (Speedex; Colten, Swiss) index was developed Incise edge to a height of 2 mm diamond bur (, GA Savannah 004348U0, Brasseler USA,) was shaved and Finish Line Inter facial Contact Prvgzyma Lee was placed proximal region of burs disc size limiting cutting depth 0.3 mm (013210U0, Brasseler USA) and 0.5 mm (013212U0, Brasseler USA) to determine the depth of the diamond cutting. The milling (004864U0, Brasseler USA) was used to complete the CNC lathe with milling and polishing applications (000584U0, Brasseler USA) supplemented. Other dental veneer laminate was used as the cutting edge incisal except that after a short amount of 2 mm cutting the lingual surface in this area was expanded by creating a chamfer margin (30).
Beveled teeth with Silicone molding material (Speedex; Colten, Swiss) with acrylic molding and mold epidural (GC pattern Resin; GC Grop, Tokyo Japan) were dumped.
The Finish Line on Two master metal die permanently identified.
Points A and B on the labial surface Points D and E on the lingual surface Points C and F on each proximal surface Of each metal die with a more specific (light polymerized Hanan-wolfgang, Germany) with Relief mm3, the Silicone material (Speedex; Colten, Swiss) 30 times done molding . Format with a stone (Silky-Rock; whip miscopy, Louisville) Type IV were cast. Dies for the final setting time was 24 hours. Margin was examined under a stereomicroscope with a magnification of 20 to have any Trays. Then dies Estonia currently 60 different designs with cutting laminate there (30 dai by cutting 2 mm incisal edge and shoulder pattern in the area and the Finish Line 30 die by cutting 2 mm chamfer on the lingual incisal edge with extension form) then dies in any of the groups into two groups, divided into 15 packages (19, 20, and 22, 27 and 28). The first group to build laminate veneers fled spastic [Duceram; Degu Dent, Hanau-Wolfgung, Germany) was used as follows. The second group was used for making veneer Inceram laminate follows. First, with the silicon die [Dubliermass; Vita Zohnfabrik, Germany] Rfrktvry molding and die with the [stumpfmass; Vita Zohnfabrik, Germany] were cast.
At this stage blind separation from the die, the material separator [Insulation Gel; Vita Zohnfabrik, Germany] was used. Core material [spinell MgAl2O3; Vita Zohnfabrik, Germany] was applied on the die. Dies in a porcelain furnace to a temperature of 1100 ° C were then sintered cores were obtained At this stage, the use of porous core material [Spinell Glass Powder; Vita Zahnfabrik, Germany] porcelain ovens were infiltrated and again, but at this point the furnace temperature is raised to 1130 ° C to prepare a solid core. Then, Porcelain [Vita VM7; Vita Zahnfabrik, Germany] took the blind man. For fixing veneers Finish on the master steel die in this study to assess the mismatch margin of the die-adhesive, [Ducera lay super fit; Degut Dent, Hanau-wolf gang, Germany] was used as the material for bonding conventional fled spastic porcelain laminates during the manufacturing process used to die. The material, color and consistency of honey, cream and Film thickness is very low, which makes use of very small amounts of a strong but reversible binding between the metal and laminates for die to be the each use, a metal die washed with water, dried, and subsequent re-evaluation of marginal adaptation veneer is an extremely small amount smeared on the die (31).
 |
Figure 1: Labial surface of a Duceram and a Inceram veneers under a stereomicroscope |
Gap Assessment Methodology Gap Assessment margin, measured with computerized digital image analysis system was used. This set includes a stereomicroscope [Stereoscopic Zoom microscope; Nikon Corporation, TokyD, Japan] digital camera (Digital Sight Camera Nikon, tokyd, Japan) are the stereomicroscope the camera images on a computer monitor will do, form vivid images laminates and metal die junction margin on monitor with Resolution software.It should be noted that the measurements were repeated three times at each point.
Research by Holmes (32) the vertical distance between the inner surfaces of the outer edge of the margin to the Finish Line steel die is considered as a marginal gap. Using Soft Camera DS-LS)) that the monitor was distributed.
Results
In this study, two-way analysis of variance (two way ANOVA) to examine the main effects (type CNC lathe and various parts of the laminate) and interaction (type CNC milling various parts of × × type laminate) is used(Tab-1). Results show significant differences depending on the cutting gap is found. But the gap in various areas cutting rates show significant differences (p <0.01). Rate gap based on the type of laminate had a significant difference (p <0.05).
The tests also indicate that the level of interaction Gap (12 effects) is also significant (p <0.01).(Tab-2)
Table 1: two-way analysis of variance (two way ANOVA) to examine the main effects and interaction in marginal gap
| Source | Sum of squares | Degrees of freedom | Mean squares | F | P value |
| Type of CNC | 2513.327 | 1 | 2513.327 | 2.392 | .124 |
| Preparation areas | 161800.603 | 2 | 80900.302 | 77.006 | .000 |
| Type of laminate | 1145033.207 | 1 | 1145033.207 | 1.090E3 | .000 |
| Type of CNC× lathe parts × type of laminate | 405211.899 | 7 | 57887.414 | 55.101 | .000 |
| Error
|
179648.389 | 171 | 1050.575 | ||
| Total | 8733516.928 | 183 |
Check out 12 shows that the interaction effect (chemfer × Labial × Duceram) the extent and effect of gap = 383.59 ± 35.75 (sholder × Labial × Duceram) gap = 364.1 ± 48.16, significantly highest rate gap in values between 12 of their work. The three works, (chamfer × Labial × In Ceram) the amount of gap = 97.06 ± 36.27 (shoulder × Labial × In Ceram) the amount of gap = 101.23 ± 20.6 (shoulder × Proximal × In Ceram) gap = 98.8 ± 29.1 at a rate significantly significant gap between the lowest values are 12 types of effects.
Table 2: The Don chon test indicate that the level of interaction Gap (12 effects) is also significan
| Type of CNC | Preparation areas | Type of laminate | Total | Average |
| chemfer | Labial | Inceram | 15 | 97.06 f ± 36.27 |
| Duceram | 15 | 383.59 a ±35.75 | ||
| Lingual | Inceram | 15 | 142.39bd ±36.15 | |
| Duceram | 15 | 208.48 c ±36.3 | ||
| Proximal | Inceram | 15 | 103.87 ef ±36.52 | |
| Duceram | 15 | 255.08 b ±36.6 | ||
| sholder | Labial | Duceram | 15 | 364.10 a ±48.16 |
| Inceram | 16 | 101.23 f ±20.6 | ||
| Lingual | Duceram | 15 | 177.53 cd ±24.95 | |
| Inceram | 16 | 150.09 d ±15.8 | ||
| Proximal | Duceram | 15 | 254.24 b ±19.2 | |
| Inceram | 16 | 98.80 f ±29.11 |
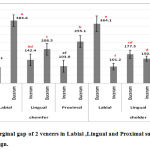 |
Figure 2: Bar chart-1:Marginal gap of 2 veneers in Labial ,Lingual and Proximal surfaces according to marginal design. |
Discussion
Increasing advances in technology make it possible to allow the use of dental prostheses without the metal scene. But the prerequisite for success in any healing process is an exact match prosthesis remaining tooth structure (33). Based on the results of present study we carried that the level of the margin gap that feldspathic porcelain laminate veneers Du ceram system are not blind about the clinical μm 273 which is non-negligible, but the laminate veneers In ceram the inner core, rate gap margin around μm 115 was based on the study Mclean (1971) which showed the degree of mismatch edge to μm 120 in clinical is acceptable), seems to lack marginal in Duceram according to findings (1990 ) Hung SH (28) shrinkage and shrinkage porcelain firing cycle is over. They show that non-uniform deformation of porcelain during the firing phase correction, matching porcelain crowns without affecting the blind. However, the results Hilgert (2003) identified the correct baking In ceram porcelain system does not lead to a marginal reduction. In their study on the marginal adaptation of In ceram internal system 40 copping onto two metal have been finishing line chamfer and shoulder were calculated, then copping both groups under the two types of processes were sandblasting the statistical analysis was shown that the marginal adaptation of coping does not change the results of both studies confirmed our study (34).
Amount of marginal gap for laminate veneers In ceram in this study μm 115 which as of Sulaiman (1996) (27) (level of mismatch marginal μm 66/160) and also of Gray (1993) (35) (level of mismatch edge the porcelain of in ceram μm) 123) and the study Yeo (2003) (4) where μm 112, there is the possibility to evaluate the marginal adaptation of metal Mstrday use laminate veneers and veneers Du ceram in ceram system without having to cementing a laminate made possible on the die. In this research, including studies Rinke (1995) (36) and Groten (1997) (29) Sulamian (1997) (27) and Nakamure (2000) (37) and Tinschere (2001) (38) Gap Measurement margin before cement samples were evaluated.
Reference
- Fernado Z, Ettore E, Giuliana L, Roberto S, Marco F. (2006). Dynamometric assessment of the mechanical resistan of porcelain veneers related to tooth preparation: A Comparision between two techniques; J Prosthet Dent , 95:35-36.
- Schmidt k, ChiayabutrY, PhillipsK, KoisJ.(2011). Influence of preparation design and existing condition of tooth structure on load to failure of ceramic laminateveneers; J Prosthet Dent 2011,105:374-382.
- Strassler HE. (2007). Minimally invasive porcelain veneers: indication for a conservative esthetic dentistry treatment modality. Gen Dent , 55(7): 686-94.
- Yeo IS, Yang JH, Lee JB. (2003). In vitro marginal fit of three all- ceram crown systems. J Prosthet Dent , 90:459-64.
- Biodl A, Mormann WH.(2005). Marginal and internal fit of all-ceramic CAD/CAM Crown copings on chamfer Perparations. J Oral Rehabil , 32:441-7.
- Rinke S, Huls A, Jahn L. (1995). Marginal accuracy and fracture strength of conventional and copy milled all- ceramic crowns . Int J Prosthodont, 8:303-10.
- Christensen GJ. (1966). Marginal fit of gold inlay casting. J Prosthet Dent , 16:297-305.
- Mclean JW, Von Franunhofer JA.(1971). The estimation of cement film thickness by an invivo technique. Br Dent J, 131:107-11.
- Jacobs MS, Windeler AS. (1991). An investigation of dental luting cement solubility as a function of the marginal gap . J Prosthet Dent, 65: 436-42.
- Goldman M, Laosonthoorn P, White RR. (1992). Microleakage of full crowns and the dental Pulp. J Endod , 18:473-5.
- Tuntiprawon M, Wilson PR. (1995). The effect of cement thickness on the fracture strength of all- ceramic crowns. Aust Dent J, 40: 17-21.
- Martin G, Delef A, Heiner W.(2000). Determination of minimum number of marginal gap measurements required for practical in vitro testing . J Prosthet Dent, 83:40-9.
- Lopes G, Baratier Luiz, Andrada M. (2001). All-ceramic post, core and crown : Technique and case report. J Esthet Restor Dent , 13: 285-95.
- Ferrari M, Patroni S, Balleri P. (1992). Measurment of enamel thickness in relation to reduction for etched laminate veneer. Int J Periodontics Restorative Dent , 12(5): 407-13.
- Kuda WH. (2000). Using a modified subopaquing technique to treat highly discolored dentition. JADA , 131(7): 945-950.
- Frederick M, Robert A, Robert J. (1993). Marginal gap width of a new refractory porcelain system. J Prosthet Dent , 69:564-7.
- Heather J, Wook- Jin S, Igor J. (2007). Current ceramic materials and systems with clinical recommendations A systemic review. J prosthet Dent, 98:389-404.
- Pera P. Gilodi S, Bassi F, Carossa S. (1994). In vitro marginal adaptation of alumina porcelain ceramic crowns. J Prosthet Dent, 72: 585-90.
- Baig M, Tan K, Nicholl J. (2010). Evaluation of the marginal fit of a zirconia ceramic computer- aided machined (CAM) crown system . J Prosthet Dent , 104:216-27.
- Quintas AF, Oliveria F, Bottino MA. (2004). Vertical marginal discrepancy of ceramic copings with different ceramic materials, finish lines, and luting agents: an in vitro evaluation. J Prosthet Dent , 92:250-7.
- Davis DR.(1988). Comparision of fit of two types of all-ceramic crowns. J Prosthet Dent, 59:12-16.
- Balkaya MC, Cinar A, Pamuk S.(2005). Infolunce of firing cycles on the margin distortion of 3 all ceramic crown systems. J Prosthet Dent , 93:346-55.
- Vigolo P. Fonzi F. (2008). An in vitro evaluation of fit of zirconium oxide based ceramic four- unit fixed partial dentures, generated with three different CAD/CAM systems, before and after porcelain firing cycles. J Prosthot Dent, 17:621-6.
- Reich S, Kappe K, Teschner H. (2008). Clinical fit of four- unit zirconia posterior fixed dental prostheses. Eur J Oral Sci, 716:579-84.
- Goldin EB, Boy d NW, Goldstein GR. (2005). Marginal fit of leucite glass pressable ceramic restorations. J Prosthet Dent, 93: 743-7.
- 26.Gonzalo E, Suarez MJ, Serrano B. (2009). A comparison of the marginal discrepancies of zirconium and metal ceramic fixed dental prostheses before and after cementation. J Prosthet Dent , 102:378-84.
- Sulamian F, Jameson LM, Wozniak WT. (1997). A comparison of the marginal fit of Inceram , IPS Empress , and procera crowns. Int J Prosthodont, 10:478-84.
- Hung SH, Hung KS, Eick JD. (1990). Marginal fit of porcelain fused to metal and two types of ceramic crowns. J Prosthet Dent, 63:26-31.
- Groten M, Axmann D, Probster L. (2006). Determination of the minimum number of marginal gap measurements required for practical in vitro testing. J Prosthet Dent , 95:315-22.
- Lin T, Liu P, Ramp L, Essig M, Givan D.(2012). Fracture resistance andmarginal discrepancy of porcelain laminate veneers influenced by preparation design and restorative material in vitro; j o u r n a l o f d e n t i s t r y,40:202-209.
- Soares CJ, Martins LRM, Ferandes AJ. (2003). Marginal adaptation of in direct composites and ceramic Inlay systems. Operative Dentistry, 28-6: 689-694. 32. Holmes R, Bayne S, Salik D.(1989). Consideration in measurement of marginal fit.J prosthet Dent1989 ; 62:405-8.
- Christensen GJ. (1999). Porcelain fused to metal vs non metal crowns. J Am Dent Assoc, 130:409-11. 34. Hilgert E, Nesser M. (2003). Evaluation of the marginal adaptation of ceramic copings in function of the cervical endings and treatment of the internal surfaces. Ciens odontal Bras, 6:9-16
- Grey NJ, Piddock V, Wilson MA. (1993). In vitro comparison of conventional crowns and a new all ceramic system. J Dent , 21: 47-51.
- Grey NJ, Piddock V, Wilson MA. (1993). In vitro comparison of conventional crowns and a new all ceramic system. J Dent , 21: 47-51.
- Nakamura T, Nonaka M, Marayama T. (2003). In vitro fitting accuracy of copy milled alumina cores and All ceramic crown. Int Prosthod, 13(3): 189-93. 38. Tinschert J, Natt G, Maustsch W. (2001) . Marginal fit of alumina and zirconia based fixed Partial denturs produced by a CAD-CAM system. Oper Dent; 26(4): 367-74.
- Chan C, Harazthy G, Geis- Gerstorfer J. (1985). The marginal fit of cerestore full ceramic crown a preliminary report. Quintessence , Int : 16:309-402.

