
Manuscript accepted on :
Published online on: --
Plagiarism Check: Yes
Ali Reza Kabiri* and Farhang Farokhi Nejad
School of Medicine, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
DOI : https://dx.doi.org/10.13005/bpj/883
Abstract
Acute appendicitis is one of the most important and common causes of acute abdominal pain in patients admitted to the emergency department of hospitals. Diagnosis of this disease in people admitting with abdominal pain is not simple. On the one hand, delay in diagnosis is the most important factor of in increasing mortality in these patients. This study aims to investigate the Alvarado scores in acute appendicitis patients hospitalized in an emergency department. This is a retrospective cross-sectional study conducted on 480 patients (354 male, 126 female) diagnosed with acute appendicitis and underwent appendectomy in a surgical ward. Patients with identical Alvarado scores were placed in separate groups and the diagnostic accuracy of each score (1 to 10) was calculated for all patients based on age gender. To evaluate the diagnostic accuracy of Alvarado scoring in both genders compared with the total population, Independent T sample test was used. In addition, the appendix phase was extracted by the information available in the file. From the Alvarado scores - in the total study population - tenderness with 16.99% (480/476 patients), and temperature rise with 37.39% (480/189 patients) had the lowest frequency. This amount (sensitivity of Alvarado score > 6) was 6.89%, and 3/87% in men and women, respectively. No statistically significant difference in diagnostic sensitivity was observed in any of the above groups. In investigation patients for appendix phase, supportive phase had the highest frequency. Our findings show that Alvarado scoring system can be used as a proper diagnostic method in the diagnosis of acute appendicitis. In addition, it was shown that supportive phase had the highest frequency.
Keywords
Acute appendicitis; Appendectomy; Alvarado score
Download this article as:| Copy the following to cite this article: Kabiri A. R, Nejad F. F. Evaluation of Alvarado Score in Acute Appendicitis Patients Hospitalized in the Emergency Department of A Hospital During 2008- 2009. Biomed Pharmacol J 2015;8(2) |
| Copy the following to cite this URL: Kabiri A. R, Nejad F. F. Evaluation of Alvarado Score in Acute Appendicitis Patients Hospitalized in the Emergency Department of A Hospital During 2008- 2009. Biomed Pharmacol J 2015;8(2). Available from: http://biomedpharmajournal.org/?p=6202 |
Introduction
Acute appendicitis is the most common cause of abdominal pain and its diagnosis can be difficult especially in the early stages of the disease. In addition, significant morbidity and mortality was occasionally observed in patients, which may be due to errors in well timed diagnosis of the disease [1]. The overall mortality rate in acute perforated appendicitis is also approximately 3% (or 50 times higher). The mortality rate of perforated appendicitis in the elderly is approximately 15% (5 times higher than the overall rate) [6]. Currently, the main method of appendicitis diagnosis is clinical method and laboratory tests such as white blood cells count and their percentage differences helps to the diagnosis [2]. Currently, the main method of appendicitis diagnosis is clinical method and laboratory tests such as white blood cells count and their percentage differences helps to the diagnosis. History and physical examination are the most effective diagnostic methods [3]. Basic organisms observed in natural appendicitis, acute appendicitis, and perforated appendicitis is Escherichia coli and Bacteroides fragilis. However, there may be many types of optional and anaerobic bacteria and mycobacteria [6]. There are different scoring systems based on signs and symptoms of the patient to evaluate acute abdominal pain. MANDRELS scoring system was proposed by Alfredo Alvarado in 1986 [4]. This scoring system is based on clinical and laboratory criteria.
From 1983 to 2000, nineteen studies have been conducted aiming to devise rating ways to diagnose appendicitis or check diagnostic accuracy of the innovated rating methods using laparoscopic imaging. Teicher et al. (1983) proposed using rating techniques for the diagnosis of acute appendicitis, and by comparing the two groups with positive and negative appendectomy surgery, showed that by using the rating methods, the normal appendectomy surgery would be reduced to a third rank [5].
The MANDRELS scoring system was proposed by Alfredo Alvarado to facilitate the diagnosis of acute appendicitis in 1986. This scoring system is based on clinical and laboratory criteria. These criteria include: Pain shift, anorexia, nausea, and vomiting, right lower quadrant of the abdomen tenderness, rebound tenderness, temperature rise, leukocytosis, and shift to the left. In this scoring system, tenderness in the right lower quadrant of the abdomen and leukocytosis receive score two and the others received score one, that will be a total of 10 scores. He concluded that patients with score six and higher would be more likely suffering from appendicitis. This study aims to evaluate the sensitivity of this scoring system in acute appendicitis diagnosis and its relationship with appendix phase.
Materials and Methods
This is a retrospective study based on the data present in the patients’ records. Alvarado signs and symptoms were investigated from the medical history records of the patients. In this study, white blood cell count greater than 11,000, and the presence of more than 75% neutrophils have been considered as leukocytosis (in adults), and shift to the left, respectively. Appendix phase was extracted from the surgical resident’s description in the file. All data was entered in SPSS system edition 15. Patients with identical Alvarado scores were placed in separate groups and the diagnostic accuracy of each score (1 to 10) was calculated in the total study population and each gender. To evaluate the diagnostic accuracy of Alvarado scoring in both genders compared with the total population, Independent T sample test was used. In this study, the chi-square statistical test has also been used to investigate the relationship between Alvarado score and appendix phase.
Results
Total of 480 patients (354 men, 126 women) with acute appendicitis that underwent appendectomy surgery were studied. From the Alvarado scores-in the all study population – tenderness with 16.99% (480/476 patients), and temperature rise with 37.39% (480/189 patients) had the lowest frequency. In the entire study population, Alvarado score > 7 had diagnostic sensitivity of 72.5%, and Alvarado score> 6 had diagnostic sensitivity of 89%. The sensitivity to Alvarado score (> 6) in men and women was 6.89% and3.87%, respectively. No statistically significant difference in diagnostic sensitivity was observed in all of the above groups. In the studied patients for appendix phase, supportive phase had the highest frequency.
From the Alvarado scores – in the all studied population – tenderness with 476 patients (16.99%), and temperature rise with 189 patients (37.39%) had the lowest frequency. The frequency distribution of Alvarado scores for different clinical and pathological parameters of the disease is presented in Table 1:
Table 1: The frequencydistribution of Alvarado scores for different symptomsin the all patients
| Tenderness | 99.16 % | 476 |
| Anorexia | 94.16% | 452 |
| Rebound | 88.75% | 426 |
| Pain shift | 80.62% | 387 |
| Vomiting | 79.37% | 381 |
| Leukocytosis | 66.25% | 318 |
| Shift to the left | 62.08% | 298 |
| Temperature rise | 39.37% | 189 |
From the Alvarado scores in men, tenderness (43.99%) had the highest frequency, and temperature rise (27.39%) had the lowest frequency. The frequency of Alvarado scores are presented in Table 2:
Table 2: The frequency distribution of Alvarado scores for different symptomsin men
| Tenderness | 43.99% | 352 |
| Anorexia | 94.36% | 334 |
| Rebound | 89.84% | 318 |
| Pain shift | 82.21% | 291 |
| Vomiting | 78.25% | 277 |
| Leukocytosis | 65.82% | 233 |
| Shift to the left | 61.3% | 217 |
| Temperature rise | 39.27% | 139 |
From the Alvarado scores in women, tenderness (42.98%) had highest frequency, and temperature rise (69.39%) had the lowest frequency. The frequency distribution of the Alvarado scores in women is presented in Table 3:
Table 3: The frequency distribution of Alvarado scores for different symptoms in women
| Tenderness | 98.42% | 124 |
| Anorexia | 94.45% | 119 |
| Rebound | 85.72% | 108 |
| Vomiting | 82.54% | 104 |
| Pain shift | 76.2% | 96 |
| Leukocytosis | 68.26% | 86 |
| Shift to the left | 64.29% | 81 |
| Temperature rise | 39.69% | 50 |
Table 4: The frequency distribution of Alvarado scores (1 to 10) in the men.
| Score | Number of patients | Percent (%) |
| Score 3 | 5 | 1.4% |
| Score 4 | 10 | 2.8% |
| Score 5 | 22 | 6.2% |
| Score 6 | 51 | 14.4% |
| Score 7 | 54 | 15.3% |
| Score 8 | 48 | 13.5% |
| Score 9 | 119 | 33.7% |
| Score 10 | 45 | 12.7% |
The highest obtained score in men was 10, and the lowest score obtained was 3. Scores 1, and 2 have not been observed in any patient. Score 9 with 7.33% of cases and score 3 with 1/4% of cases have the highest and lowest frequency, respectively. According to the chart above it can be seen that score 10, total scores of 9 and 10, score > 8, score > 7, and score > 6 have the diagnostic sensitivity of 12.7%, 46.4%, 59.9%, 75.2%, and 89.6%, respectively.
Independent T test analysis showed no significant difference in the frequency distribution of the Alvarado scores in males, compared with total population (P = 0.54).
Table 5: The frequency distribution of the Alvarado scores (1 to 10) in women
| score | Number of patients | Percent (%) |
| Score 4 | 2 | 1.6% |
| Score 5 | 14 | 11.1% |
| Score 6 | 28 | 22.2% |
| Score 7 | 15 | 11.9% |
| Score 8 | 11 | 8.7% |
| Score 9 | 37 | 29.4% |
| Score 10 | 19 | 15.1% |
The highest score obtained in women was 10, and the lowest score obtained was 4. Scores 1, 2, and 3 have not been observed in any patient. Score 9 with 4.29% of cases and score 4 with 6.1% of cases have the highest and lowest frequency, respectively. According to the chart above it can be seen that score 10, total scores of 9 and 10, score > 8, score > 7, and score > 6 have the diagnostic sensitivity of 15.1%, 44.5%, 53.2%, 65.1%, and 87.3%, respectively. According to p> 0.05 in Independent T sample test, no significant difference was observed in the frequency of the Alvarado score in males, compared with total population (P = 0.54).
In the total study population, patients who got the score 6 or higher were 427 cases, from which 317 were males and 110 were females.
The frequency distribution of appendicitis phase was investigated in the studied population (Fig. 1.)
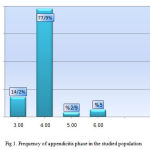 |
Figure 1: Frequency of appendicitis phase in the studied population |
As it can be seen in Figure 1, late supportive phase with 9.77% (374 patients) is the most prevalent. Early supportive phase, perforated phase, and gangrene phase include 14.2% (68 patients), 5% (24 patients), and 9/2% of cases (14 patients), respectively.
In a study conducted in American Alexandra Hospital, Alvarado score ≥7 had the sensitivity of 77%, which is consistent with our study [12]. In a study by Shepherd in Vincent Health Center of America the Alvarado score ≥ 7 had the sensitivity of 77 % that is consistent with the sensitivity of this study [9]. In Kenman and Khan (2005), conducted in at the Khyber Teaching Hospital in Peshawar, Pakistan, the diagnostic sensitivity score ≥7, 84.3% is mentioned. This rate has been reported 88% in men, and 1.82% in women. Statistics of this study are consistent with our study [10]. In Sharivastava, Gupta, and Sharma (2004) conducted in Guru Teg Bahadur Hospital in Delhi, Alvarado score ≥ 6 had 92% sensitivity. In addition, this rate was 84% for men, whichis consistent with our study [11].
In Owen et al. (1994) conducted in Waltz University Hospital in America, Alvarado score ≥ 7 had the sensitivity of 94%, and 87% in men and women, respectively.
Appendix 1: Alvarado scoring for diagnosis of appendicitis
| Criterion | Score | ||
| Symptoms | |||
| Pain shift | 1 | ||
| Anorexia | 1 | ||
| Nausea and Vomiting | 1 | ||
| Symptoms | |||
| Tenderness RQL | 2 | ||
| Rebound | 1 | ||
| Temperature rise | 1 | ||
| In vitro symptoms | |||
| Leukocytosis | 2 | ||
| Shift to the left | 1 | ||
| Total scores | 10 | ||
Conclusion
In general, our study population had Alvarado score ≥ 6, and diagnostic sensitivity of 89%. This rate was 89.6%, and 87.3% in men and women, respectively. No statistically significant difference in diagnostic sensitivity was observed in any of the above groups compared with the total study population. In addition, it was shown that the development of the appendix phase does not create a significant increase in increased sensitivity of Alvarado system.
According to the convenient diagnostic accuracy of Alvarado scoring system in males and females and also due to the simplicity and low costing of this method and that it can be done quickly, Alvarado scoring system can be used as a convenient diagnostic method in cases of doubt to acute appendicitis.
Due to the high sensitivity of score 6, it is recommended that patients who receive score 6 or higher in Alvarado scoring system to be moved to the operating room to undergo appendectomy, and patients with a score less than 6 are expected to receive treatment.
References:
- Alvarado A. A practical Score for the early diagnosis of acute appendicitis . Ann Emerg Med 1986؛ 15:557-65
- Kaiser S، Jorulf H، Soderman E، Frenckner B، Impact of radiologic Imaging on the surgical decision-making process in suspected appendices in children. Acar radio 2004؛11:971-9
- Ohmann C، Franke C، yang Q. Clinical benefit of diagnostic score for appendicitis: result of a prospective interventional study. German study group of acute abdominal pain. Arch Surg 1999؛ 134:993-996
- Alvarado A. A practical score for the early diagnosis of acute. Appendices. Ann Emerg Med 1986؛15:557-64.
- Teicher I, Landa B, Cohen M, Kabnick LS, Wise L. Scoring system to aid in diagnoses of appendicitis. Annals of surgery. 1983;198(6):753.
- Kessler N، Cyteval C، Gallix B، Lesnik A، Blayac PM، Pujol J، Appendicitis: evaluation of sensitivity ، specificity، and predictive values of US، Doppler Us، and laboratory findings. Radiology 2004؛ 230:472-8.
- Bernard M، Jaffe and david H، The appendix. In:F Charles Brunicardi، Dana K Anderson، Timothy R. Biller، David l. Dunn، John G Hunter، Raphael E. Pollock Schwartz’s Principles of surgery. Teimourzadeh puplicao n، 2005.
- Abdl Ghani Soomro, Faisal Ghani Siddiqui, Arshad Hussain Abro, Shahnawaz Abro, Noshad Ahmed Shaikh and Abdul Sattar Memo. Diagnostic Accuracy of Alvarado Scoring System in Acute Appendicitis. JLUMHS MAY – AUGUST 2008u.
- . Baidya N, Rodrigues G, Rao A, Ahmed Khan S. Evaluation Of Alvarado Score In Acute Appendicitis: A Prospective Study.Internet J of Surg 2007; Vol 9, No 1.
- Mckay R، Sheoherd J. The use of clinical scoring system by Alvarado in the decision to perform computed tomography for acute appendicitis in the ED. Am J Emerg Med 2007 jan25(5):489-93.
- Khan I, Kenman A. Application of Alvarado scoring system in diagnosis of acute J Avud Medical Abbot abed 2005.17(3):41-4.
- Sharivastava UK, Gupta A, Sharma D, Evaluation of Alvarado score in diagnosis of acute Appendicitis. Iran Med J.2004 25(4):184-6.
- M Y P Chan B S Teo, B L Ng,The Alvarado score and Acute appendicitis, ann Acad Med Singapore
- T D Owen H Williams, G Stiff , L R Jenison B I Rees University Hospital of Wales Heat Park, Cardiff . Evaluation of Alvarado Score in Acute Appendicitis. Journal of Royal Society of Medicine volume 85 February 1992.p 87-88
- Khan A . S Rao and Rodrigues , A Baidya,G. Citation:N. Evaluation of Alvarado Score In Acute Appendicitis: A prospective Study. The Internet Journal of Surgery.2007 Volume 9 Number 1.
- Kirtland E. Hobler, MD Acute and Suppurative Appendicitis: Disease Duration and its Implications for Quality Improvement. The Permanente Journal ,Spring 1998 Volume 2No.2.5-8

