
Manuscript accepted on :
Published online on: 23-12-2015
Plagiarism Check: Yes
R. Balakrishnan, Vijay Ebenezer and Abu dakir
Department of Oral and Maxillofacial Surgery, Sree Balaji Dental College and Hospital, Bharath University, Chennai, 600 100, India.
DOI : https://dx.doi.org/10.13005/bpj/480
Abstract
The treatment of mandibular fractures has evolved from various forms of wiring, splinting, intermaxillary fixation, rigid fixation, compression plates, and mini plates. But in all this circumastances there is a chance of potential infection and malunion in mandibular fracture site. So in our study we used three dimensional titanium miniplates to stabilize the mandibular fracture site. The 3 D titanium miniplates stability and fixation and adaptibilty yielded better results than the conventional miniplates.
Keywords
Mini plates; Mandibular fracture site; 3D titanium miniplates
Download this article as:| Copy the following to cite this article: Balakrishnan R, Ebenezer V, dakir A. Three Dimensional Titanium Mini Plates in Management of Mandibular Fractures. Biomed Pharmacol J 2014;7(1) |
| Copy the following to cite this URL: Balakrishnan R, Ebenezer V, dakir A. Three Dimensional Titanium Mini Plates in Management of Mandibular Fractures. Biomed Pharmacol J 2014;7(1). Available from: http://biomedpharmajournal.org/?p=2933 |
Introduction
Over the years, the management of trauma has evolved from various forms of splinting circum mandibular wiring (R.J.Fonseca&R.V.Walker) extra-oral pins, semi rigid fixation and trans-osseous wiring. This was followed by rigid fixation technique and more lately has given way to semi-rigid fixation with miniplates (Champy.M.et al)3,10,11 . The currently used conventional miniplates technique requires maxillomandibular fixation for a short period and unable to render three dimensional stability at the fracture site2, 12.At times it is highly desirable to effect a method of fracture reduction which will provide rapid bone healing18, mechanical stability and obviates the use of inter-maxillary ligation. The three dimensional (3-D) miniplate system is one of the recent internal rigid fixations for the maxillomandibular surgery in years8.The three dimensional plating system is based (Farmand 1993)9 on the principle of obtaining support through geometrically stable in the three-dimensions of the fracture site since it offers good resistance against torque forces.
Material and Methods
All the patients were managed by rigid internal fixation using, Titanium three dimensional miniplates. The patients were operated under local or general anesthesia by appropriate approach to the fractured site, either by intra-oral or extra-oral method1. Patients were included on the basis of the following criteria.
Any fracture of the mandible at the symphysis, parasymphysis, body, angle region subcondylar region and especially in those cases where fracture fragments were badly displaced where closed reduction was not sufficient enough to reduce the fracture.
Malunited or non-united cases of fracture mandible in above-mentioned area.
Fracture of the mandible with edentulous posterior fragments, which presents difficulties with regarding to closed reduction.
 |
Figure 1
|
 |
Figure 2
|
 |
Figure 3
|
 |
Figure 4
|
Results and Observations
The present study was conducted in six patients having fractured mandible with a total no of twelve fractures sites. All the patients were treated with locking 3D titanium miniplates..
Table 1: Shows the sex wise distribution of the patients in the present study. The maximum patients in the present study were 67% males while 33% female.
| Gender | No of patient | Percentage |
| Male | 4 | 67% |
| Female | 2 | 33% |
| Total | 6 | 100% |
Table 2: Shows the age wise distribution of the patients in our study. All the patient in this study were in the age group of 23-56 years. In our study age group distribution is same in all groups.
| Age Group | No of Patient | Percentage |
| 20-29 years | 2 | 33% |
| 30-39 years | 2 | 33% |
| 40 & above | 2 | 33% |
| Total | 6 | 100% |
Table 3: Gives an idea about the etiology of fracture. The road traffic accident was responsible for majority of cases (50%). In 33% patient, fracture was occurred because of assault and in 17% patient fracture resulted due to fall.
| Etiology | No of Patient | Percentage |
| Road traffic accident | 3 | 50 % |
| Assault | 2 | 33 % |
| Miscellaneous fall Etc | 1 | 17 % |
| Total | 6 | 100% |
Table 4: shows the different anatomical location of fracture mandible revealed that parasymphysis (58%) is the most common site followed by Subcondyle region (25%) and angle (17%).
| Fracture site | No of Patient | Percentage |
| Symphysis | 0 | 0% |
| Parasymphysis | 7 | 58% |
| Angle | 2 | 17% |
| Body | 0 | 0% |
| Subcondyle | 3 | 25% |
| Total | 12 | 100% |
Discussion
Farmand 19928 developed the concept of 3-D mini plates. Their shape is based in the principles of quadrangle as geometrically stable configuration for support. Since the stability achieved by the geometric shape of these plates surpasses the standard mini-plates, the thickness can be reduced to 1 mm. The basic form is quadrangular with 2×2 hole square plate and 3×2 rectangular plate.
The 3-D mini plates itself was a misnomer as the plates themselves were not 3 dimensional, but holds the fracture segments rigidly by resisting the 3 dimensional forces namely shearing, bending and torsional forces occurring on the fracture site in function17.
 |
Figure 5
|
 |
Figure 6
|
The previous studies in the use of the 3-D titanium miniplate for mandibular fracture treatment, reported low complication rates and studies concluded that the 3-D mini plate is a predictable alternative to conventional mini-plates5,14.
The advantage is easy application, which avoids a time consuming extra oral approach and associated complications15.
Another advantage is simplified adaptation to the bone, without distortion (or) displacement of the fracture, as well as the simultaneous stabilization at both the superior and inferior borders, making the 3-D mini plates a time saving alternative to conventional mini plates (Feledy et al.)13
One more advantage of 3-D plates is the improved biomechanical stability compared with conventional mini-plates.
It has been claimed that mobility of fragments is a causative factor in the post operative infection because infection is the most common complication in mandibular fracture, the improvement of plate stability might minimize the problem. With the use of open reduction and internal fixation, the reported incidence of infection ranges from 3%-32%. Infection rates in the clinical studies in 3-D miniplates are 5.4%-9%.
All patients with mandibular Fractures were treated with 3-D titanium mini plates of which 2 fractures treated with 3×2 hole 3-D plate and 10 fractures with 2×2 hole 3-D mini plate with extra oral and intra oral approaches.
In our study, 50% of mandibular fractures were caused due to Road Traffic Accidents. It can be explained by the fact that there are no comprehensive rules for traffic safety as there are in western countries. These need to be formulated and strictly enforced.
Inter personal violence caused 33% of the mandibular fracture in our study and miscellaneous causes like fall, sports accounted for the remaining 17%. This correlated with the study carried out by ( Rowe & killey 1968).
Out of the total 12 fractues, Parasymphysis region had the maximum incidence 58%, Subcondylar had 25% and the angle fracture had the minimum incidence of 17%.
Dr. Champy had done the study and reviewed that mandible is the weakest in the parasymphysis region because of presence of teeth and curvature of body of the mandible that makes it an easy target in fights. And falls on the other hand, the bone is very dense at the symphysis.
The present study showed that the 3-D titanium plate allows no movement at the superior and inferior borders with maximal torsional and bending forces as opposed to a single linear plate applied to superior border area.
When only one linear plate is placed at the superior border area, torsional and bending forces usually cause movement along the axis of the plate with bucco-lingual splaying and gap formation at the inferior border respectively. In 3-D titanium plate system the screws are placed in the box configuration on both sides of fracture rather than on a single line and broad platform is created that may increase the resistance to torsional forces along the axis of the plate4,5.
Because of the design of the 3-D plate is conceptually that of two linear plates connected by reinforcing vertical struts. Strut plates may therefore provide greater resistance against gap opening at the inferior border with biting forces compared to a single plated applied at the external oblique ridge or superior lateral border.
All cases were treated by standard extra oral and intra oral approaches. In this tissue dissection is done only in the vicinity of the planned osteotomy or fracture line. The 3-D plates are positioned such a way that the horizontal bar is perpendicular and the vertical bar is parallel to the fracture line.
In recent days the use of 3-D plating has secured a place, helping the surgeon to use it with ease16. Where ever fixation is necessary. The following advantages of this 3-D system made it a successful armamentarium in mandibular fixation cases.
The only probable limitation of these plates may be excessive implant material due to the extra vertical bars incorporated for countering the torque forces.
Advantages of the Technique
Minimal tissue dissection near the osteotomy and fracture line
Fixation point remains in vicinity of osteotomy line.
Stability of the 3-D plate obtained by its configuration not by thickness or length
Blood supply to the fragments is not disturbed.
Adjustments are easy because of thin connecting arms of the plate.
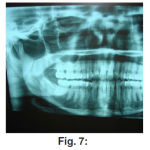 |
Figure 7
|
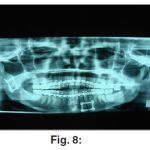 |
Figure 8
|
Summary
The surgical technique and instrumentation used in this study were in accordance with the established technique of miniplate osteosynthesis.
A Majority of the patients in the study were males (67%).Road traffic accidents (RTA) being the most common cause (50%). Parasymphysis fractures had the highest incidence among the fractures (58%).
No post-operative Maxillo-mandibular fixation was done in any of the patients. Follow up was done up to a period of 6 months. One patient reported complication of infection at the extra-oral site, which was successfully managed with conservative measures and did not require surgical intervention.
The results of our study were put to comparison with previous studies on fracture mandible and were found to be in accordance with them6,7,15. All the patients in our study appreciated early recovery of normal jaw function, primary healing and good union at the fracture site with minimal weight loss due to early reinstatement of the masticatory function. There was great patient acceptance of this treatment plan.
During the course of our study the three – dimensional titanium miniplates were found to be standard in profile, strong yet malleable, facilitating reduction and stabilization at both the superior and inferior borders giving three dimensional stability at fracture site.
Hence, we conclude from our study that 3-D titanium mini plate system may be considered as a viable treatment option for mandibular fracture management.
Reference
- A. W. Sugar et al: A randomized controlled trial comparing fixation of mandibular angle fractures with a single miniplate placed either transbuccally and intra-orally, or intra-orally alone. Int. J. Oral Maxillofac. Surg. 2009; 38: 241–245
- Bjorn Johanson et al: “Miniplate osteosynthesis of infected mandibular fractures.” Jr. Cr. Maxillofacial Surg.16, (1998), 22-27.
- Champy: “Mandibular osteosynthesis by mini plates via buccal approach.” J of Max. Fac. Surg. 6,14,1978.
- Conor P. Barry: Superior Border Plating Technique in the Management of Isolated Mandibular Angle Fractures: A Retrospective Study of 50 Consecutive Patients. J Oral Maxillofac Surg 65:1544-1549, 2007.
- Constantin A. Landes,et al: Bone and Plate Fixation Device for Trans-oral Osteofixation in the Mandibular Angle, Ramus, and Condyle Region. © 2007 American Association of Oral and Maxillofacial Surgeons 0278-2391/07/6510-0038$32.00/0.
- Edward Ellis III: Treatment of mandibular angle fractures using two 2.4 mm dynamic compression plates Jr. Oral Maxillofacial Surg. 51(1993)969-973.
- Edward Ellis III: Use of lag screws for fractures of the mandibular body Jr. Oral Maxillofacial Surg. (1996)54, 1314-1316.
- Farmand M, Dupoinrieux L: The value of 3-dimensional plate in maxillofacial surgery. Rev: stomatol chir maxillfac.1992:93(6):353-357.
- Farmand: The 3-D plating system in maxillofacial surgery, AAOMSp.166-1993.Abstract session 16.
- T. Jacson: The use of champy mini-plates for osteosynthesis in craniofacial deformities trauma. Jr. Plast & Recon.Surg. (1986) 77, 5:729-736.
- Juergen Zix et al: Use of Straight and Curved 3-Dimensional Titanium Miniplates for Fracture Fixation at the Mandibular Angle. J.Oral Maxillo fac Surg 65:1758-1763, 2007.
- Manoj Kumar Jain et al: Comparison of 3-Dimensional and Standard Miniplate Fixation in the Management of Mandibular Fractures. J.Oral Maxillofac. Surg. 68:1568-1572, 2010.
- Farmand et al: The treatment of fractured edentulous maxilla. Jr.Cran.Maxillofacial Surg. 20(1992),341-344.
- Farmand: Three dimensional plate fixation of fractures and osteotomies. Jr.Facial plastic surgery clinics of North American vol.3.No.1.Feb.1995, page 39-56.
- Hughes et al: 3D plate verses the lag screws technique for treatment of fractures of the anterior mandible. ADOMS; 2000:23-24.
- Robert M. Kellman: Recent advances in facial plating technique. Jr.Fac.Plast. Clinics of North America. Vol. 3. No. 3. (1995).
- J et al: A three-dimensional study of bending and torsion moments for different fracture sites in the mandible. Int.J.Oral Maxillofacial.Surg.1997; 26: 383-388.
- Vivek Shetty et al: Fracture Line Stability as a Function of the Internal Fixation System. Jr.Oral Maxillofacial Surg. 53; 791-801 (1995).

