
Manuscript accepted on :
Published online on: 23-12-2015
Plagiarism Check: Yes
R. Balakrishnan, Vijay Ebenezer and Abu Dakir
Department of Oral and Maxillofacial Surgery, Sree Balaji Dental College and Hospital, Bharath University, Chennai, 600100, India.
DOI : https://dx.doi.org/10.13005/bpj/484
Abstract
The topic of condylar injury in adults has generated more discussion and controversy than any other in the field of maxillofacial trauma. It is an important subject because such injuries are common and complications of trauma to the temporomandibular joint (TMJ) are far-reaching in their effects.The aim of this paper is to report one of such cases. A 15 yr male patient reported to our department with a chief complaint of inability to close mouth. On examination and radiographs the case was diagnosed as left sub condylar fracture and dento-alveolar fracture of anterior maxillary segment. The case was posted for operation under GA. And the dento alveolar fracture to be treated with Arch Bar and left sub-condyle fracture by open reduction and internal fixation.
Keywords
Management; Sub Condylar; Fracture
Download this article as:| Copy the following to cite this article: Balakrishnan R, Ebenezer V, Dakir A. Management of Sub Condylar Fracture in 15 yr Old Patient : Case Report. Biomed Pharmacol J 2014;7(1) |
| Copy the following to cite this URL: Balakrishnan R, Ebenezer V, Dakir A. Management of Sub Condylar Fracture in 15 yr Old Patient : Case Report. Biomed Pharmacol J 2014;7(1). Available from: http://biomedpharmajournal.org/?p=2947 |
Introduction
Considering the relatively benign, possibly adverse, consequences of condylar fractures (eg, jaw dysfunction, temporomandibular joint (TMJ)/muscle pain, and malocclusion), and the relatively difficult procedures required for open reduction (compared with reduction of a mandibular angle or symphysis fracture), there will always be a difference of opinion among surgeons concerning the merits of open versus closed reduction. The incidence of condylar process fractures among all mandibular fractures is high, most likely in the range of 25% to 50%. For decades, “conventional wisdom” has suggested
that closed reduction of mandibular condyle fractures has been the preferred approach to treatment. This widely held belief has been fostered by such statements as “complications arising from fractures of the mandibular condyle are conspicuous by their absence.” While cutting edge research at present reveals completely different interpretations when scrutinized by today’s standards. A recurring theme of Brandt and Haug(1) is the demonstration of a high rate of complication and treatment failure after closed reduction.
An evaluation of 382 patients with condylar process fractures by Silvennoinen et al(2) found that
84% were unilateral/l6% bilateral; 2) 14% were intracapsular; 3) 24% were condylar neck; 4) 62% were subcondylar (low neck/ramus); and 5) 16% were categorized as having severe displacement (MacLennan’sclassification)(3). When analyzed by age group, 41% of the fractures in children 10 years or younger were judged to be intracapsular, whereas 70% were subcondylar in the 20- to 29-year age group, and 66% were subcondylar in the 30- to 39-year age group. Sixty percent of the fractures occurred in the 20- to 39-year age range. There is much concern about ankylosis following condylar process fractures, but the actual incidence is very infrequent and probably only 0.4% at most.(4)
Children between 12 and 18 years still benefit from their growth potential following closed reduction, but have fractures similar to adults (ie, more low neck/ramus) due to the mandible reaching adult shape(5). Thus, open reduction, with rigid fixation and immediate function is a strong option in this age range.(6)
There are three general philosophies of surgeons toward management of subcondylar fractures of the mandible in patients 12 years and older.(7)
Closed treatment or observation is done for all fractures regardless of the amount of condylar displacement. Most patients do well without anatomic alignment. For those few patients who develop a problem that they consider a disability, (eg, malocclusion, ankylosis, painful jaw movement), surgery can be performed secondarily to correct the problems, eg, by osteotomy or joint replacement.
Open reduction is done for severely displaced (or dislocated condyles) that are torn loose from normal joint attachments (capsule, disc) and lie in a position outside the normal area of condylar translation. The rationale for this philosophy is that, although the great majority of fractures do well without open reduction, the patients with severely displaced condyles have a greater likelihood of developing a problem that will be considered a disability, and thus the risk, effort, and expense of open reduction is justified for regaining anatomic bony alignment”(8)
Open and closed reduction treatment are considered equally for all patients, the final procedure being determined by such variables as level of fracture, displacement, presenting occlusion and function, finances, and the patient’s desires(9). The philosophy is that open reduction with rigid internal fixation in many cases allows for the best possibility of returning the patient to the pretrauma condition rapidly without a period of maxillomandibular fixation (MMF) or interarch guiding elastics, and minimizes functional or occlusal changes for which the patient would have to develop compensatory habits, or need further treatment.(10,11)
Enthusiasm for open treatment of condylar process fractures has increased over the past 20 years with the wide availability of plate and screw fixation systems(12). While there may be good reasons to perform this surgery, a prerequisite is that it can be safely performed. With any skeletal fracture, the biology of the components must be understood to assure that one can reduce the fracture and provide stability to the components without undue harm.(13)
To determine whether or not open treatment of condylar process fractures is biologically sound, one must first determine:
The blood supply to the condyle.
Whether or not the blood supply is essential to open treatment.
 |
Figure a
|
Case Report
A male patient aged 15 yrs reported to our department with a chief complaint of inability to open mouth and disturbed occlusion following road traffic accident 5 days back. He presented with a laceration in the lower lip which was sutured primarily in a Primary Health Centre. He was also given injection tetanus toxoid, Antibodies and Analgesics. For definitive management, the case was referred to our institute.
On examination the patient presented with a deviated and restricted mouth opening. Deviation was towards the left side. There was a laceration in the lower right side of the lip, which was sutured. There was also reduced ramus height on the left side. Intra-orally there was presence of fractured upper anterior teeth. There was total non occlusion on the right side.
On palpation left pre auricular region had mild depression accompanied with pain. The prominence of the condyle is not felt. Upper anterior maxillary segment had a slight mobility from canine to canine region with intrusion of upper right lateral incisor. The patient also complained inability to completely close his left eye.
The pre operative OPG reveals subcondylar fracture with displacement on the left side. Also there was dento alveolar fracture of the upper anterior.
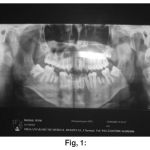 |
Figure 1
|
 |
Figure 2
|
After case discussion it was decided to treat the condylar fracture with open reduction and fixation. And dentoalveolar fracture with archbar.
The case was admitted in Sree Balaji Medical college and posted for surgery following complete blood investigations and fitness.
Under GA Alkayat Bramley incision marking was done on the left side and incision was done.
 |
Figure 3
|
Skin and fascia flap was raised above the temporal fascia till the level of zygomatic arch. The Glenoid fossa was identified and “T” incision was placed over the joint capsule to expose the joint.
 |
Figure 4
|
After exposure of the glenoid fossa was found to empty. The condyle was found to be displaced medially. And the Mandibular Ramus was inferiorly.The condyle was freed from its connective tissue attachments except on the medial side.
 |
Figure 5
|
The condyle and mandibular segments were re approximated and reduced anatomically
After proper reduction was achieved, Fixation was done with 4 hole mini plate. The mouth opening was checked and the occlusion was stabilised temporarily with IMF. The joint capsule was re- approximated and sutured with 2-0 vicryl
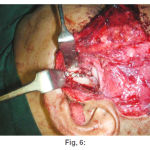 |
Figure 6
|
 |
Figure 7
|
The skin and fascia flap was closed in 2 layers with 2-0 vicryl and 3-0 ethilon. Pressure bandage was applied over the surgical site.
 |
Figure 8
|
The IMF was released after 2 days and the patient was advised mouth opening exercises. He showed a good mouth opening of 3 fingers.
 |
Figure 9
|
 |
Figure 10
|
Conclusion
Fractures of the mandibular condyles constitute a notable portion of mandibular fractures. A number of clinical signs and symptoms should alert the clinician to the possibility of such injuries. The use of plain radiographs in multiple views usually discloses most condylar fractures, although the advent of the CT scan has made a more definitive and detailed evaluation and description of these injuries possible. There has been resurgence in literature supporting open reduction and internal fixation of condylar fractures, citing improved condylar stability and occlusal results, earlier return of joint function, and improved cosmesis(13). Knowledge of regional anatomy and improved techniques for surgical access to the TMJ has greatly reduced complication rates(14). There are a number of surgical approaches to the condylar fracture and an equal number of different methods of reduction and fixation of the fracture segments(15). The simplest method with the least complications based on the specifics of the fracture (location, type of fracture, displacement of segments, age of the patient and concomitant medical conditions) should be used.
References
- Brandt MT, Haug RH: Open versus closed reduction of adult mandibular condyle fractures: A review of the literature regarding the evolution of current thoughts on management. J Oral Maxillofac Surg 61:1324, 2003
- Silvennoinen U, Iizuka T, Lindqvist C, et al: Different patterns of condylar fractures: An analysis of 382 patients in a 3-year period. J Oral Maxillofac Sure 50:1032. 1992
- MacLennan W: Consideration of 180 cases of typical fractures of the mandibular condylar process. Br J Plast Surg 5:122, 1952
- Matthew B. Hall :Condylar Fractures : Surgical Management. J Oral Maxillofac Surg 52:1189-1192,1994
- Tateyuki Iizuka,Kurt Liidrach, Alfred H. Geering,Joram Rave: Open Reduction without Fixation of Dislocated Condylar Process Fractures: Long-Term Clinical and Radiologic Analysis, / Oral Maxillofac Surg 56:553-561, 1998.
- Hovinga, G. Boering, B. Stegenga: Long-term results of nonsurgical management of condylar fractures in children. Int. J. Oral Maxillofac. Surg. 1999,” 28: 429-440. _9 Munksgaard, 1999.
- Matthew B. Hall :Condylar Fractures : Surgical Management. J Oral Maxillofac Surg 52:1189-1192,1994
- MacLennan W: Consideration of 180 cases of typical fractures of the mandibular condylar process. Br J Plast Surg 5:122, 1952
- Edward Ellis III and Gaylord S. Throckmorton: Occlusal Results after Open or Closed Treatment of Fractures of the Mandibular Condylar Process, J Oral Moxillofoc Surg 58 260-268.2000.
- Leon A. Assael, Open Versus Closed Reduction of Adult Mandibular Condyle Fractures: An Alternative Interpretation of the Evidence. J Oral Maxillofac Surg 61:1333-1339, 2003.
- RudolfR.M. Bos, Fractures of the Condylar Process: Surgical Versus Nonsurgical Treatment, J Oral Maxillofac Surg 57:397-398, 1999
- Pedro M. Villarreal, Florencio Monje, Luis M. Junquera, Jesu´s Mateo, § Antonio J. Morillo, and Cristina Gonza´lez, Mandibular Condyle Fractures: Determinants of Treatment and Outcome.
- Dongmei He, Edward Ellis III, Yi Zhang: Etiology of Temporomandibular Joint Ankylosis Secondary to Condylar Fractures: The Role of Concomitant Mandibular Fractures, 2008 American Association of Oral and Maxillofacial Surgeons J Oral Maxillofac Surg 66:77-84, 2008.
- Vitomir S. Konstantinove & Branislav Dimitrijevic: Surgical Versus Conservative Treatment of Unilateral Conciyiar Process Fractures: Clinical and Radiographic Evaluation of 80 Patients. J Oral Maxillofac Surg 50:349-352, 1992.
- C. A. Landes, R. Lipphardt: Prospective evaluation of a pragmatic treatment rationale: open reduction and internal fixation of displaced and dislocated condyle and condylar head fractures and closed reduction of non-displaced, non-dislocated fractures. Part II: high condylar andcondylar head fractures. Int. J. Oral Maxillofac. Surg. 2006; 35: 115– 126.#2005 International Association of Oral and Maxillofacial Surgeons.

