
Manuscript accepted on :
Published online on: 18-12-2015
Plagiarism Check: Yes
Abdolrasool Moloudi*, Alireza Ray and Babak Heidari
Emam Ali Heart Hospital, Shahid Beheshti Blvd., Kermanshah, Iran.
DOI : https://dx.doi.org/10.13005/bpj/406
Abstract
Acute stent thrombosis is one of the most important complications of percutaneous coronary intervention (PCI). It is recommended to use anticoagulant drugs to prevent this disease. At present heparin is the most commonly used drug in this field. However, it is used less than intravenous enoxaparin (low molecular weight heparin). In this clinical trial, these two drugs are used during PCI in patients and early nosocomial complications of each of them are considered and evaluated. This study was conducted during 1387-1388 on 304 patients divided into two groups of E (Enoxaparin) and H (Heparin) consisting of 150 patients each. Patients were hospitalized in CCU (Intensive Care Unit) for 48 hours and were evaluated after PCI in terms of acute nosocomial complications. The results of this study are analyzed using T-Test and Logestic Regression. In this study was conducted on 304 patients with an average age of 55±9. Major bleeding, acute vascular occlusion and death were observed in none of these two groups. Minor bleeding and local hematoma in group H are more significantly different from those in group E (p>0.05). 64% and 51% drug-eluting stent was used in groups E and H, respectively. Statistical analysis showed no significant difference between these two groups in terms of drug-eluting stents (p>0.05). In group E, sheath was removed up to one hour after the PCI procedure, while it lasted 7 hours in group H (P=0.000). The present study showed that there is no significant difference between the acute nosocomial complications in PCI patients and the kind of anticoagulant medicine. However, the duration of arterial sheath removal in group E was significantly lower than that in group H.
Keywords
Percutaneous Coronary Angioplasty (PCI); Heparin; Enoxaparin; Early Complications
Download this article as:| Copy the following to cite this article: Moloudi A, Ray A, Heidari B. Comparing Therapeutic Effect of Enoxaparin and Intravenous Heparin therapy in Percutaneous Coronary Intervention (PCI). Biomed Pharmacol J 2013;6(2) |
| Copy the following to cite this URL: Moloudi A, Ray A, Heidari B. Comparing Therapeutic Effect of Enoxaparin and Intravenous Heparin therapy in Percutaneous Coronary Intervention (PCI). Biomed Pharmacol J 2013;6(2). Available from: http://biomedpharmajournal.org/?p=2695 |
Introduction
500,000 PCIs is performed in America annually, and the use of this treatment is spreading all over the world as well as Iran [1]. Over the past three decades, continuing advances have occurred in medical equipments of PCI and the use of drug-eluting stents and have provided conditions for treating patients with complex coronary arteries complications. One of the problems of stent placement inside coronary is trombogencity of this device. Besides association with the type, length and diameter of stent, trombogencite is directly associated with predisposing factors for coronary artery disease (CAD) such as diabetes; It is recommended to use intravenous heparin during the procedure and aspirin and clopidogrel before and after the procedure to prevent acute stent thrombosis. Using this treatment, acute vascular occlusion is reduced to less than 3% of existing cases [2]. Of course, Colombo et al. disagree severe anticoagulation of patients and believe that this approach increases patients’ mortality [3]. Several studies have reported acute vascular occlusion and acute coronary events after PCI (Percutaneous coronary intervention) in both drug and non-drug eluting stents the same, and their early results are almost the same [4, 5].
Limitations in using heparin especially anticoagulation (nonlinear) effect of this drug and its negligible effect on factor Xa have led to the use of enoxaparin (a type of low molecular weight heparin (LMWH)) instead of heparin in some studies. Although the use of enoxaparin is recommended for treating patients with unstable angina and its advantages are proved [6-8], there is no agreement over the prescription of intravenous enoxaparin during PCI procedure. This drug binds to plasma protein to a lesser extent and has better bioavilibity and more anti-factor Xa effect compared to HMWH.
Considering the above-mentioned advantages, todays enoxaparin is extensively used in treating patients with acute coronary events, and the present study aims to compare therapeutic effects of heparin and enoxaparin in patients undergoing PCI, and acute complications of this disease are evaluated during hospitalization [7, 9].
Materials and Methods
In this clinical trial, patients referred to hospital and candidate for PCI are divided into two groups of E and H using convenience sampling regardless of demographic characteristics such as age, gender, weight, type of vessel involved. Group E included patients receiving intravenous enoxaparin during the procedure, and Group H included patients receiving intravenous heparin. Patients with emergency PCI, coronary thrombotic lesions, diabetes or impaired renal function (serum creatinine>2 or platelets< 100,000) were excluded from the study.
Pre-procedure cares included ECG, echocardiogram, CPK and troponin I, coagulation tests and platelet counting. All patients were hospitalized in CCU after the procedure, and their coagulation tests and cardiac biomarkers were checked 12-24 hours after the procedure. All patients were asked to provide a written consent for PCI, but they were not informed of the kind of anticoagulant drug. However, interventionists were aware of the type of anticoagulant drug.
The average heparin dose prescribed during the procedure was 10,000 units in group H (100 u/k). The prescribed dose of intravenous enoxaparin was. On completion of the procedure, sheath was removed from femoral artery after controlling ACT and PTT in both groups. Before PCI, all patients received aspirin and Plavix (clopidogrel). The size of arterial sheath used in all patients was 6 (size=6). Homeostasis lasted for at least 10 minutes in both groups. Then pressure dressing was done. Transferring patients from catheterization center to CCU, all of them were monitored, electrocardiography was performed every six hours, cardiovascular markers of CPK and troponin were checked every 12 hours, patients were carefully examined for the incidence of chest pain and Cardiac arrhythmia and every ST-segment changes in electrocardiography, and information were recorded in the designed checklist [10].
Local and severe bleeding, femoral region hematoma, acute vascular occlusion, acute myocardial infarction (AMI), and nosocomial mortality were among data recorded in patients’ checklists. Having an stable clinical condition and lacking any problems or mentioned complications, all patients were discharged from the hospital 48 hours after intervention (angioplasty). Information collected from evaluated patients included age, gender, weight, type of vessel involved, the number of vessels involved and type of applied balloon and stent. In addition, acute complications of PCI during 24 hours were accurately followed and evaluated.
Sample Size, Sampling Method and Data Analysis
Sample size was studied considering the results of similar studies with 90% confidence coefficient and 80% power of the test. 152 patients were considered as sample size for each group and a total of 304 patients were evaluated.
All analyses were performed using Stata statistical software (version 8). Qualitative data of both groups were analyzed and compared using descriptive statistics (frequency) and finally X2 test. Quantitative data were presented using mean and standard deviation and were finally compared using T-Test. X2 test and Fisher’s exact test (if necessary) are used to compare complications such as local bleeding, hematoma, acute vascular occlusion, acute myocardial infarction (AMI), and need for blood transfusion in the two groups. In addition, Multiple Logistic Regression is used to control confounding variables and to determine the independent effect (from background variables) of the type of therapy (heparin – Enoxaparin) on various study complications.
Results
304 patients aged 42-70 (with an average age of 55±9) including 210 males and 94 females were studied during 1387-1388. There were 103 (67/1%) and 108 (71%) males in groups E and H, respectively. In group E, 63 patients (41/4%) had a history of myocardial infarction (MI) , and 102 patients (67/1%) had a history of unstable angina (UA). In group H, 80 (52/6%) and 112 (73/6%) patients had a history of MI and UA, respectively.
Major bleeding, acute vascular occlusion and death were observed in none of the two groups. However, minor bleeding and local hematoma occurred in both groups statistical analysis showed a significant difference between the two (p<05/0). In addition, a case of transfusion (0/6%) and AMI was observed in group E, although statistical analysis showed no significant difference with group H (p=0.314). Furthermore, the increase in cardiac arrhythmias and electrocardiographic changes showed that group E is not significantly different with group H in these two cases (transfusion and AMI) (Figure 1).
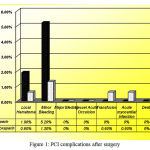 |
Figure 1: PCI complications after surgery
|
64% and 51% drug-eluting stent was used in groups E and H, respectively. Statistical analysis showed no significant difference between these two groups in terms of drug-eluting stents (p>0.05).
T-test analysis showed a significant difference between the two groups in terms of sheath removal duration. In group E, sheath was removed up to one hour after the PCI procedure, while it lasted 7 hours in group H (P=0.000) (Figure 2).
Discussion
At present, scientific criteria recommend using low molecular weight heparin instead of standard unfractionated heparin [11-13], however the use of enoxaparin in PCI is still being considered [14].
The present study aims to compare the therapeutic effect of enoxaparin and intravenous heparin in PCI. Findings of this study showed that major adverse cardiac event (i.e. major bleeding and acute vascular occlusion and death) were observed in none of the two groups. The present study is consistent with studies conducted by Korovesis et al. showing the two groups were not significantly different after surgery in terms of major adverse cardiac events [15]. Studies conducted by Keriaks at al. showed the same incidence of complications in both groups [14], and studies conducted by Galeotes.G et al. reported a 2% (vs. %8/2) reduction in bleeding in group E [16].
However, group H showed more cases of local hematoma and minor bleeding and this difference was also statistically significant. Although transfusion and AMI was observed in group E, only one case of MI was NSTEMI compared to group H. this was due to the closure of Side Branch, but has created no statistically significant differences between the two groups.
Sheath removal duration in group E was 6 hours less than that in group H. In a study conducted by Choussat, Sheath removal duration was 4 hours after surgery and patients showed no severe complication [17]. However, in the study conducted by Korovesis et al., they removed sheath immediately after surgery. The sooner the arterial sheath is removed, the less hospitalization and hospital costs would be [15].
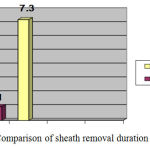 |
Figure 2: Comparison of sheath removal duration
|
However, it seems that the sheath removal duration is directly related to enoxaparin dose used. In this study, the dose used was being equal to the dose used in Korovesis’s study. In both studies, the increase in dose caused to remove sheath sooner than standard and primary times. While the dose used in Choussat’s study was and consequently the sheath removal duration was longer [17]. But it should be noted that the higher the dose of used enoxaparin, the higher the incidence of side effects of PCI would be. Therefore, the use of complementary and alternative drug-eluting stents is recommended. This justifies more use of drug-eluting stent in group E compared to group H in this study.
Conclusions
The results of this study showed that enoxaparin can be a suitable alternative to heparin in PCI. Enoxaparin not only has fewer side effects than heparin, but also the duration of arterial sheath removal is much less than that of heparin. Therefore, it is recommended to conduct further studies with different doses of enoxaparin along with different drug-eluting stents.
References
- Smund, B., et al., intravenous Enoxaparint versus unfractionated Heparin in unselelcted patients undergoing Percutaneous coronary interventinons. Euro intervention Journal 2010. 6(3): p. 407-412.
- Neumann, F., et al., Stent anticoagulation and technique. 4 ed. Textbook of Interventional Cardiology, ed. Topol. 2003, Philadelphia.
- Lefkovits, J., et al., Role of Inhibitor Agents in coronary Artery Disease, in Textbook of interventional cardiology, Topol, Editor. 2003, Elsevier Health Sciences. p. 3.
- Ferguson, J., et al., Enoxaparin vs unfractionated heparin in high-risk patients with non-ST-segment elevation acute coronary syndromes managed with an intended early invasive strategy: primary results of the SYNERGY randomized trial. JAMA: the journal of the American Medical Association, 2004. 292(1): p. 45-54.
- Moliterno, G.D., Anticoagulants and their use in Acute Coronary Syndromes and Coronary lnterventions, in Textbook of interventional Cardiology, Topol, Editor. 2003, Elsevier saunders philadelphia p. 2, 3, 33, 35, 37, 39, 56.
- Montalescot, G., et al., Enoxaparin versus unfractionated heparin in elective percutaneous coronary intervention. New England Journal of Medicine, 2006. 355(10): p. 1006-1017.
- Collet, J.P., et al., Percutaneous coronary intervention after subcutaneous enoxaparin pretreatment in patients with unstable angina pectoris. Circulation, 2001. 103(5): p. 658-663.
- Kokolis, S., et al., Anticoagulation strategies for patients undergoing percutaneous coronary intervention: unfractionated heparin, low-molecular-weight heparins, and direct thrombin inhibitors. Progress in cardiovascular diseases, 2004. 46(6): p. 506-523.
- Bhatt, D., et al., Periprocidural Myocardial Infarction and Emboli protection, in Textbook of Interventional Cardiology, Topol, Editor. 2003, Elsevier Saunders Philadelphia: Philadelphia. p. 25.
- Acheatel, R., et al., Enoxaparin vs Unfractionated Heparin in High – Risk Patients with Non ST-Segment Elevation Acute Coronary Syndromes Managed With an Intended Early Invasive Strategy JAMA: the journal of the American Medical Association, 2004. 292: p. 45-54.
- Braunwald, E., Application of current guidelines to the management of unstable angina and non-ST-elevation myocardial infarction. Circulation, 2003. 108(16 suppl 1): p. 28-37.
- Bonow, R.O., et al., Unstabre Angina and Non -ST- Erevation Myocardial Infarction in Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine, Cannon and Braunwald, Editors. 2008, Elsevier Health Sciences: Philadelphia.
- Popma, J.J., et al., Antithrombotic Therapy During Percutaneous Coronary Intervention The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. CHEST Journal, 2004. 126(3_suppl): p. 576S-599S.
- Kereiakes, D.J., et al., Low–molecular-weight heparin therapy for non-ST-elevation acute coronary syndromes and during percutaneous coronary intervention: An expert consensus. American heart journal, 2002. 144(4): p. 615-624.
- Korovesis, S., et al., Comparison of enoxaparin and unfractionated heparin in coronary angioplasty. Hellenic J Cardiol, 2005. 46(1): p. 46-51.
- Galeote, G., et al., Use of a combination of enoxaparin or unfractionated heparin and abciximab during percutaneous coronary interventions: a randomized pilot study. Revista Española de Cardiología, 2002. 55(12): p. 1261-1266.
- émi Choussat, R., et al., A unique, low dose of intravenous enoxaparin in elective percutaneous coronary intervention. Journal of the American College of Cardiology, 2002. 40(11): p. 1943-1950.

