
Manuscript accepted on :
Published online on: 14-12-2015
Plagiarism Check: Yes
Vijay Ebenezer, R. Balakrishnan, M. Vivek and M. Elumalai*
1Department of Oral and Maxillofacial Surgery, Sree Balaji Dental College and Hospital, Bharath University, Chennai - 600 100, India.
2Department of Pharmacology, Sree Balaji Dental College and Hospital, Bharath University, Chennai - 600 100, India
Abstract
The aim of this paper was to review the efficacy of ringer’s lactate solution in treatment of Temporomandibular joint ( TMJ ) disorder, especially those with closed lock. Arthrocentesis is a simple and minimally invasive procedure in treating patients with this disorder who failed to respond to conservative measures. Ringers lactate solution under sufficient pressure is used to wash out the joint inflammatory cells and to release the stuck disc phenomenon. This has been a boon for both the patient and the clinician in treating this disorder. It is cost effective and safe with minimal morbidity. This review paper has been described about Ringer’s Lactate in treatment of TMJ disorder
Keywords
Arthrocentesis; Ringer’s Lactate; Temporomandibular Joint disorder; Closed Lock
Download this article as:| Copy the following to cite this article: Ebenezer V, Balakrishnan R, Vivek M, Elumalai M. Usage of Ringer’s Lactate Treatment in Temporomandibular Joint Disorder. Biomed Pharmacol J 2012;5(2) |
| Copy the following to cite this URL: Ebenezer V, Balakrishnan R, Vivek M, Elumalai M. Usage of Ringer’s Lactate Treatment in Temporomandibular Joint Disorder. Biomed Pharmacol J 2012;5(2). Available from: http://biomedpharmajournal.org/?p=2538 |
Introduction
The temporomandibular joint is a movable diarthroid synovial joint which is formed by mandibular condyle and temporal bone. The joint space is divided into two compartments by articular disc. The upper compartment allows translation of the condyle. The lower compartment allows rotation movement of the jaw around its axis, through both the condylar heads – a hinge joint. Various etiology have been described for the TMJ disorders, posing a challenge to the clinicians treating them. The treatment modalities ranging from non – surgical to surgical interventions have been advocated for variety of diseases. The important progress in the treatment of TMJ disorder is the use of arthroscopy. Arthroscopy is found useful for both diagnostic purpose and therapeutic procedures by the use of TMJ arthroscopic lysis and lavage.1
Arthrocentesis is a simple and cheapest alternative to arthroscopic surgery2,3. This procedure can easily be done in outpatient under Local Anesthetic without using any arthroscope. This technique is very specialized and patients have a very good and quick recovery phase. 4Brennan (2006) advocated that the use of intra articular morphine injection with arthrocentesis have given good results. 5Ercument Onder (2009) have conclude that long term cure using arthrocentesis was found to be useful . The idea is to wash out the joint inflammatory cells in the jaw joint which causes the pain & restricted jaw 6 . Steroids may also be instilled into the jaw joint depending on the severity of the condition.
Arthrocentesis is a simple and a specialized technique using sterile needles and sterile irrigants to carry out the joint wash out. Ringer’s lactate is one of the irrigants used for this purpose. Since Ringer’s lacate is comparitively closer to human serum it is preferred to other irrigants used for this purpose. The patients with TMJ disorders present with sudden onset of pain in TMJ region, presence or absence of clicking with jaw movements, limited jaw movements because of pain associated with temporomandibular joint.
Discussion
The use of Ringer’s Lactate in arthroscopic lysis and lavage of the superior joint space in reestablishing the normal jaw function has gained much recognition in recent times and it is thought that the concept of arthrocentesis evolved from these procedures. This mode of treatment has shown remarkable success rate despite not using major surgical interventions. This minimally invasive surgical procedure has gained much recognition in the recent times. Murakami et al(1995),7 while being the first to document a systematic description of the procedure, also reported a high success rate in treating patients with temporomandibular joint disorders using this procedure.
2Nitzan et al (1991) described this as a simplified form of arthroscopic lavage and lysis of the joint . The studies conducted by Nitzan et al., (1991)2 and 8Frost, (1999) showed a success rate of 91% in 17 cases while Forst et al., suggested that this procedure is safe with minimal complications. The procedure proved reliable in patients with acute TMJ locking, others with chronic or osteoarthiritic cases as well as patients with a history of jaw joint surgeries, did not show such satisfactory results.
1Ohisini, (1975) described the use of the arthroscopy of the TMJ disorder. Since then various modifications and improvement in the techniques have refined the treatment of the TMJ disorders. 9Hosaka et al. (1996) have reported 78.9% success rate with arthrocentesis in patients with painful closed lock of TMJ while Murakami et al in 1995 have reported a 70% success rate in their study. 10Dimitroulis et al (1995) also have reported a significant improvement in such patients.
Internal derangement of Temporomandibular Joint varies from, clicking accompanied with normal mouth opening to clicking with restricted mouth opening (closed lock).
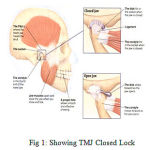 |
Figure 1: Showing TMJ Closed Lock |
11Nitzan, (1994) has reported that arthrocentesis is a turning point in treating TMJ disorders. He attributes the success of the procedure to arthroscopic lysis and lavage and hydraulic pressure used in the upper joint compartment. This procedure was found to be highly effective in restoring the normal jaw function and maximum mouth opening. 1Ohisini, (1975) have suggested that the effectiveness of this approach was due to release of the trapped, anteriorly displaced disc by the basic arthroscopic instrumentation, thereby enabling its repositioning.
Changes in the upper joint compartment may be a causative factor in limitations in condylar movements, which causes this closed lock 11,12,13. This restriction in translation of the upper joint space may just be secondary to articular surface disturbances itself. Although a variety of TMJ disorders can be treated with the arthrocentesis, documented data is mostly available in favor of closed lock 12.
14Alkan and Etoz (2010) and 15Al Belsay (2007) described that the insertion of needles for arthrocentesis is similar to arthroscopic procedure. The posterior extent of the joint space is marked 10mm forward and 2 mm down from the tragus canthal line, whereas the anterior extent is marked 10mm further forward and 10mm down from this line. Sterile irrigation solution like ringer’s lactate, normal saline or hartmann’s solution is used for this purpose, 16,17. The composition of the solution has no effect in influencing the result of the procedure. The idea of this procedure is to distend the joint and cause lavage without altering the structure or position of the disc. Release of the negative forces, reduction in the surface friction and release of the stuck disc phenomenon also, have been attributed to the possible correction of the jaw joint disorder.
18Christopher schott (2010) has been reported Ringer’s Lactate is isotonic with blood and generally used for intravenous administration. It grouped under Crystalloids. The osmolarity is 273mOsm/L. The solution contains calcium chloride , potassium chloride sodium chloride and sodium lactate
Table 1: Comparison of irrigants to human serum
Parameters Human serum (0.9%)NaCl Ringer’s lactate Albumin%
|
Na+ (mmol/l) K+(mmol/l) Ca2+(mmol/l) Cl–(mmol/l) HCo3–-(mmol/l) Albumin (g/l) Na+/ Cl– ratio pH Osmolality ( mOsm/kg) |
154 ——– ———- 154 ——– ———- 1:1 5.4 308 |
131 5 2 111 29 ———– 1.8: 1 6 276 |
140 —- —— 128 ——- 50g/l 1.09:1 ———– 265 |
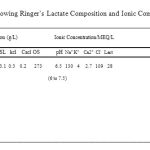 |
Table 2: Showing Ringer’s Lactate Composition and Ionic Composition |
(NaCl -Sodium Chloride, SL – Sodium Lactate, KCl – Potassium Chloride, CaCl- Calcium Chloride, Na – Sodium, K – Potassium, Ca – calcium, Cl – Chloride, Lact- Lactate, LA. Lactated, RL. Ringer’s Lactate, IUSP. Injection USP)
Since Ringer’s lactate in comparision to other irrigants is close to Human serum so, it is considered to be better tolerated by the tissues 16. 19Howard A Israle, (1999) has reported that both procedures have shown to be effective in reducing the pain and improving the mandibular movements in patients with intra articular pathological conditions.
Efficacy of the arthroscopic lysis and lavage has been described by Holmlund et al., (1994) 20. All the patients showed a significant improvement in the Maximum Mouth Opening (MMO) after the procedure. The overall success rate with MMO and the chewing ability has shown a remarkable improvement. Arthrocentesis is aimed at reducing the symptoms by removing the inflammatory cells by joint wash out21. Thereby allowing the normal cellular inflow and expediting joint repair.
Conclusion
The improvement in chewing ability and clicking of the joint post procedurally has given remarkable results. We therefore conclude that athrocentesis is helpful for those who fail to respond to the conservative treatment. There is a clear improvement in the mouth opening and pain score which encourages us to offer this treatment to the patients. Based on our review. Arthrocentesis of TMJ with Ringer’s lactate is easy, cost effective and less invasive procedure with minimal morbidity. This can be offered safely and effectively before doing more invasive procedures.
References
- ,.” Arthroscopy of temoromandibular joint.” Journal of Japanese Stomotology, 42: 207 – 13(1975)
- Nitzan, D.W., Dolwick, M. F., Martinez, G.A.”Temporomandibular joint arthrocentesis: A Simplifid traetment for sever, limited mouth opening.” Journal of Oral and Maxillofacial Surg, 49: 1163- 70 . (1991)
- Stein, J. I. “TMJ arthrocentesis. A surgical alternative”. New york state Dental Journal, 61 (9): 68 – 76.(1995)
- Brennan, P.A.” Arthrocentesis for temporomandibular pain dysfunction syndrome”. J Oral Maxillofac Surg., 64: 949 – 951(2006)
- Ercument Onder,”Long term results of arthrocentesis in degenerative temporomandibular disorder”. Oral Surg Oral med Oral pathol Oral Radiol Endod, 107: e1- e5. (2009)
- Sinan Tozoglu et al. “A review of techniques of lysis and lavage of the TMJ”. British Journal of Oral and Maxillofacial Surgery, Volume 49, Pages 302-309.(2011)
- Murakami et al,”Short-term treatment outcome study for the management of temporomandibular joint closed lock: A comparison of arthrocentesis to nonsurgical therapy and arthroscopic lysis and lavage”. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology.Volume 80, Pages 253–257. (1995)
- , D.E. “The use of arthrocentesis for treatment of temporomandibular joint disorders”. J oral Maxillofac Surg., 57; 583 – 587. (1999)
- Hideo Hosaka,KenIchiro Murakami, Kazuhisa Goto, Tadahiko Iizuka. “Outcome of arthrocentesis for temporomandibular joint with closed lock at 3 years follow-up”. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology.Volume 82, Issue 5, November, Pages 501–504 .(1996)
- Dimitroulis, G,F Dolwick, A Martinez.” Temporomandibular joint arthrocentesis and lavage for the treatment of closed lock: a follow up study”. BJOMS, 33:23 – 27. (1995)
- ”.Arthrocentesis for the management of severe closed lock of the temporomandibular Joint”. Oral and maxillofacial Surgery clinics of N. America, 6:2: 245.(1994)
- Moses, Sartoris, Glass, Tanaka.. “The effects of arthroscopic surgical lysis and lavage of the superior joint space on TMJ disc position and mobility”. Journal of Oral and Maxillofacial Surgery, 47: 674 – 78. (1989)
- McCain, P. “Arthroscopy of the human temporomandibular joint”. Jounal of Oral and Maxillofacial Surg, 40: 648 – 55. (1988)
- A., Etoz, O. “A new anatomical landmark to simplify Temporomandibular Joint arthrocentesis”. Br. Journal of Oral and Maxillofacial Surgery., 48: 310 – 1(2010)
- Al Belsay, F.A. “Arthrocentesis for thr temporomandibular Joint closed lock: A review article”. Internaltional Journal of Oral Maxillofacial Surg. 36: 773 – 782. (2007)
- Shinj, O.H., Nakata, K., Shino, K., et al. ” Effects of irrigation solution for arthroscopic surgery on intraarticular tissue. Comparision on human meniscus – primary cell culture between lactate ringer’s and saline solution”. J orthop Res, 20: 305 – 10. (2002)
- Arciero,R.A., Little,J.S., Liebenberg,S.P., Parr, T.J. “Irrigating solution used in arthroscopy and their effects on articular cartilage. An in vivo study”. Orthopedics 9(11); 1511-5. (1986)
- Christopher Schott. “Fluid Resuscitation: 0.9% Normal Saline vs Lactated Ringer’s vs Albumin”. EVMS, Journal Club Review, January 25,( 2010)
- Howard A Israle.,. “The use of arthroscopic surgery for treatment of temporomandibular joint disorders”. oral and maxillofacial surgery. 57 ;579 – 582( 1999)
- Holmmund, A., Gynther., Axelsson.. “Efficacy of arthroscopic lysis and lavage in chronic locking of the temporomandibular joint” International Journal of Oral and Maxillofacial surgery, 23: 262 – 6.(1994)
- Quinn, H., Nicolas., “Identification of prostaglandin , E2, leukoterins, B2 in the synovial fluid of painful dysfunction of TMJ.” Oral and maxillofacial surg, 48: 968 – 71.(1990).

