
Manuscript accepted on :
Published online on: 11-12-2015
Plagiarism Check: Yes
Salman Yousuf Guraya and Mohamed Adnan Zolaly
Department of Surgery, College of Medicine Taibah University, Almadinah Almunawwarah Saudi Arabia.
Abstract
There have been conflicting reports about the predictive validity of High School Grades (HSG) in determining the academic performance of the students during the medical course. The purpose of this study was to determine the predictive value of HSG in validating the academic success of the medical students in the pre-clinical and clinical years of the College of Medicine Taibah University (CMTU) Almadinah Almunawwarah Saudi Arabia. The HSG, Grade Average (GPA) of the pre-clinical and clinical years of the students entering the CMTU during the years 2004-2005 and 2005-2006 were analysed. The data were analyzed by Statistical Package for Social Sciences (SPSS, Inc., Chicago, IL, USA) version 19.0. The relation between the HSG (independent) variable and the pre-clinical and clinical GPA (dependent) variable was analyzed using Pearson’s correlation coefficient and linear regression analyses. Chi-squared statistics were applied for categorical variables. A total of 240 students (122 females and 118 males) data was retrieved for analysis. There was no statistically significant difference in HSG of male and female students but there was significant difference between the GPA of male and female students at pre-clinical and clinical in favour of the female students (P= 0.00). Chi-square analysis illustrated that GPA of pre-clinical and clinical years was not associated with the HSG. The analysis also showed a statistically significant positive correlation between the pre-clinical and clinical year performance of the entire cohort (p= 0.00). 2-tailed Pearson correlation reported no positive correlation between HSG, and pre-clinical and clinical GPA, while there was a strongly positive correlation between pre-clinical and clinical GPA at the medical school. The study concludes that HSG, considered as an important pre-admission variable in the medical school, is not a predictor of academic performance in the medical school.
Keywords
High school grades; medical school GPA; medical course; academic performance
Download this article as:| Copy the following to cite this article: Guraya S. Y, Zolaly M. A. High School Grades are not Reliable Predictors of Academic Performance in Undergraduate Medical School: A Study from a Saudi Medical School. Biomed Pharmacol J 2012;5(2) |
| Copy the following to cite this URL: Guraya S. Y, Zolaly M. A. High School Grades are not Reliable Predictors of Academic Performance in Undergraduate Medical School: A Study from a Saudi Medical School. Biomed Pharmacol J 2012;5(2). Available from: http://biomedpharmajournal.org/?p=2475 |
Introduction
The predictive validity of the various entry criteria to the medical school has been seriously challenged in the past (1). In the United States and Canada, commonly employed admission criteria include Scholastic Aptitude Test (SAT), American College Testing (ACT), Medical College Admission Test (MCAT), and High School Grades (HSG). Ever increasing demand for medical education has compelled the academia to introduce alternative methods to structure a valid, transparent, and feasible system to identify the appropriately qualified candidates for the medical courses. In order to make a holistic impression of cognitive and non-cognitive skills, additional assessment parameters have been devised. The inclusion of these alternative components of selection such as aptitude tests and some form of selection interviews has been controversial (2). The degree to which different universities rely on these three components (academic score, selection interview, and aptitude test) varies around the globe, and each university has modified the selection criteria in line with the regional needs (3).
Although HSG is a significant predictor of success in school-leaver courses, there is less certainty about the predictive value of HSG in the medical courses (4). The current study explicitly examines the predictive strength of HSG in determining the academic success of the undergraduate medical students at the College of Medicine Taibah University (CMTU) Almadinah Almunawwarah Saudi Arabia.
Methods
At the CMTU this retrospective cohort study looked into undergraduate students’ HSG, pre-clinical and clinical GPA during September through November 2012. This cohort was enrolled to the CMTU during the academic years 2004-2005 and 2005-2006 and passed out the medical course in 2010-2011and 2011-2012. The course includes a preparatory year followed by a 5-year traditional discipline-based, teacher-centered MBBS curriculum. All the students destined for Medicine, Dentistry and Pharmacy, and Allied Health sciences are admitted to a ‘common first year’ following which they are distributed to the four health sciences colleges according to their GPA and preference.
The admission criteria to the medical course at CMTU encompass HSG, a multiple choice questions exam, aptitude test score, achievement test score, and a semi structured interview. Multiple choice questions exam is conducted at various centers across the Kingdom of Saudi Arabia; ‘aptitude test’ judges the deeper understanding of given reading materials and mathematical problem-solving capabilities, and ‘achievement test’ examines the holistic scientific knowledge of three years’ of high school in chemistry, biology, physics, and mathematics, and English. Those candidates with at least 90% HSG and an average score of at least 90% in English, Physics, Chemistry and Biology are eligible to apply to the health colleges’ preparatory year program. A balanced percentage is calculated for each applicant, composed of HSG (50%), achievement test (25%) and aptitude test (25%). The candidates are finally assessed by a semi-structured interview. Such exercise looks into the communication skills, personality, and non-cognitive behavior of the candidates. No marks are dedicated to the semi structured interview and, based on overall performance, the candidates are adjudged pass or fail.
At the CMTU, first 2.5 years are dedicated to pre-clinical subjects (pre-clinical phase) while clinical disciplines are taught in the next 2.5 years of the course (clinical phase). In this study, each student’s HSG, pre-clinical GPA, and clinical GPA were analyzed. The student’s GPA is calculated by multiplying the student’s grade in each course on a 5.0 point scale by the number of credit hours for that course, then dividing this sum by the total number of credit hours taken by the student (5).
The data were analyzed by Statistical Package for Social Sciences (SPSS, Inc., Chicago, IL, USA) version 19.0. The relation between the HSG (independent) variable and the pre-clinical and clinical GPA (dependent) variable was analyzed using Pearson’s correlation coefficient and linear regression analyses. Pearson correlation coefficients were calculated with each of the predictor variables and chi-squared statistics were applied for categorical variables. A p-value of <0.05 was considered significant.
Results
The overall academic performance of the cohort of all 240 (122 male and 118 female) students showed that clinical GPA (5th year) declined from pre-clinical GPA (3rd year) and high school performance (Table 1).
Table 1; Students’ performed better in the pre-clinical (3rd year) than the clinical (5th year) component of the medical course.
| Statistics | High School Grades
|
Pre-Clinical GPA | Clinical GPA |
| No. | 240 | 240 | 240 |
| Mean | 94.75 | 3.8033 | 3.6616 |
| Median | 95.00 | 3.8900 | 3.7300 |
| Mode | 92 | 4.23 | 3.53 |
| Std. Deviation | 2.201 | .69947 | 0.58533 |
In terms of HSG, there was no statistically significant difference in performance of male and female students (Table 2). The table also illustrates a significant difference between the GPA of male and female students at pre-clinical and clinical in favour of female students (P= 0.00).
Table 2: The academic performance of the cohort in high school, and pre-clinical and clinical years of the medical school.
| Group Statistics | ||||||
| Gender | No. | Mean | Std. Deviation | t-stat | Sig. (2-tailed) | |
| High School Grades | Females | 122 | 94.72 | 2.06 | -0.24 | 0.81 |
| Males | 118 | 94.79 | 2.34 | |||
| Pre-clinical GPA | Females | 122 | 3.96 | 0.66 | 3.59 | 0.00 |
| Males | 118 | 3.64 | 0.71 | |||
| Clinical GPA | Females | 122 | 3.77 | 0.55 | 2.89 | 0.00 |
| Males | 118 | 3.55 | 0.61 | |||
Table 3 outlines the chi-square analysis of the academic performance of male and female students at pre-clinical and clinical years as compared to their high school performance. The analysis confirmed that the GPA of pre-clinical and clinical years was not associated with HSG. At the same time, the analysis showed that there was a statistically significant positive correlation between the pre-clinical and clinical year performance of the entire cohort; p= 0.00 (Table 4).
Table 3: The academic performance of the cohort comparing the high school grades with pre-clinical and clinical year GPA.
| Chi-Square Test (High school Vs pre-clinical year) | |||
| Gender | Value | Df | Asymp. Sig. (2-sided) |
| Females | 0.29 | 2 | 0.87 |
| Males | 1.31 | 2 | 0.52 |
| Chi-Square Tests (High school Vs clinical year) | |||
| Gender | Value | Df | Asymp. Sig. (2-sided) |
| Females | 0.11 | 2 | 0.94 |
| Males | 1.46 | 2 | 0.48 |
Table 4: The academic performance of the cohort comparing the GPA in the pre-clinical and clinical years of the medical school.
| Chi-Square Tests (clinical Vs pre-clinical year) | |||
| Gender | Value | Df | Asymp. Sig. (2-sided) |
| Females | 81.90 | 1 | 0.00 |
| Males | 81.41 | 1 | 0.00 |
Pearson correlation analysis suggested that there was a significantly positive correlation between GPAs of pre-clinical and clinical years, confirming that the clinical year grades were dependent on pre-clinical year grades; p = 0.00 (Table 5). The pre-clinical and clinical years’ performances were not significantly correlated with the high school performance. There was no correlation between the high school and the medical school academic performance of the students.
Table 5: Correlations between the high school, and pre-clinical and clinical years of the medical school.
| Gender | Features | High school Grades | GPA
3rd Year |
GPA
5th Year |
|
|
Females |
HSG
|
Pearson Correlation
Sig. (2-tailed) N |
1
122 |
.088
.333 122 |
.088
.338 122 |
| GPA 3rd year | Pearson Correlation
Sig. (2-tailed) N |
.088
.333 122 |
1
122 |
.954**
.000 122 |
|
| GPA 5th year | Pearson Correlation
Sig. (2-tailed) N |
.088
.338 122 |
.954**
.000 122 |
1
122 |
|
|
Males |
HSG
|
Pearson Correlation
Sig. (2-tailed) N |
1
118 |
.218*
.018 118 |
.243**
.008 118 |
| GPA 3rd year | Pearson Correlation
Sig. (2-tailed) N |
.218*
.018 118 |
1
118 |
.960**
.000 118 |
|
| GPA 5th year | Pearson Correlation
Sig. (2-tailed) N |
.243**
.008 118 |
.960**
.000 118 |
1
118 |
|
**.Correlation is significant at the 0.01 level (2-tailed).
*.Correlation is significant at the 0.05 level (2-tailed).
The scattered plots also confirmed the strongly positive correlation between the GPA of the pre-clinical and clinical years for both genders (Figure 1).
Figures 1 A and B showing the positive correlation between the academic performance of pre-clinical and clinical year for female (A) and male (B) medical students, respectively.
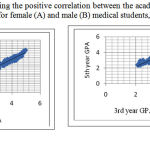 |
Figures 1: A and B showing the positive correlation between the academic performance of pre-clinical and clinical year for female (A) and male (B) medical students, respectively.
|
Discussion
The screening and selection of medical students based upon suitable criteria is a contentious issue with studies reaching different conclusions regarding the ideal model for student selection (6). At the same time, the World Association for Medical Education (WFME) recommends that the medical schools must have an admission policy including a clear statement on the process of selection of students. The admission policy should be reviewed periodically based on relevant societal and professional data (7). The CMTU has a well-structured admission criteria and HSG is an integral component of a composite admission policy.
The current study shows that the students who attained minimum academic standards at the entry level (below average HSG), are capable of reaching the standards set by the medical school regardless of their pre-admission academic performance. This confirms that HSG are not reliable predictors of academic success in the medical school. In the UK the admission of medical students mainly depends on grades achieved at school exit examination like A levels, which is equivalent to HSG in Saudi Arabia. Despite their predictive ability, A levels grades are probably not the only predictors and should not be the sole basis for selection in the medical schools (8). Three arguments have been described as fundamental parts of A levels; Achievement component which ensures a minimum competence in the sciences basic to medicine such as physiology and anatomy, an ability component because academic success mainly depends on intellectual capability, and a motivation component in the sense that A levels are effective because university education requires not only intellectual ability but also good study skills and motivation. Several studies have suggested that A level results correlated with dropout rates, career progression, post graduate membership and postgraduate royal college fellowship examination (9) (10) (11). However, other facets of a professionally sound medical graduate cannot be predicted by A levels and can be correlated with measures of personality and by learning styles (12).
Several studies have reported that female students performed significantly better overall at the end of year 2 and in year 3 of the medical schools (13) (14). These findings are consistent with the better performance of female gender at the medical school in the current study; although there was no statistically significant difference in the performance of both genders at the high school level. A growing body of published literature reports that women tend to perform better than men in their medical training (8) and are more likely to attain an honors degree.
Ferguson et al conducted a systematic review of the significant predictors of success at the medical school and concluded that, on average, previous academic performance accounted for 9% of the variance in overall performance at the medical school (15). The review examined data on the predictive validity of the eight criteria in determining the selection of medical students: cognitive factors (previous academic ability), noncognitive factors (personality, learning styles, interviews, references, personal statements), and demographic factors (sex, ethnicity). Similarly, most of the medical schools are obliged to adapt a composite screening and selection entry criteria due to pros and cons individual parameters like HSG. In the United States and Canada, the Medical College Admission Test (MCAT) is required for admission to most of the medical schools. The MCAT is computer–based assessment and tests physical and biological sciences, verbal reasoning, and writing skills (16). Donnon et al conducted a meta analysis of 23 published studies to determine the predictive validity of the MCAT for medical school performance and medical board licensing examinations and reported that the MCAT, as a total score and subtests, had small to medium predictive validity of performance in medical school during both the preclinical and clinical years (17). The MCAT total had an adjusted medium predictive validity coefficient effect size for basic science/preclinical (r _ 0.43; 18.5% of the variance) and clerkship/clinical (r _ 0.39; 15.2% of the variance). Recent reports have explored factors other than the MCAT, particularly non-cognitive ones that are associated with professionally successful physicians, as potential criteria for selection into medical school (18). Due to the multiplicity of the physicians’ roles as health-care provider, collaborator, administrator, communicator, and researcher, a challenge to the medical profession, therefore, is to develop screening and selection methods that supplement the MCAT by focusing on key personal characteristics and the complex nature of physician roles (19).
Mercer et al reported the results of a cohort study which supported combining prior academic achievement with the assessment of communication skills in a structured interview as selection criteria into this undergraduate medical course (3). The same study concluded that previous academic achievement was the most striking consistent independent predictor of success in the MBBS course. The effect of prior academic success was highest in the early academic years and diminished towards the end of the course. Such an effect of previous academic achievement matched with previous published data (20). In the present study, there was a significantly positive correlation between the academic performance of the pre-clinical and clinical GPA of the cohort (P= 0.00). The students performed better in the pre-clinical years than in the clinical years which can be explained by the unavailability of a university hospital and the difficulties encountered in the ministry of health hospitals in terms of bedside teaching, support and services given to the university staff.
The results of the present study contradict the previous report that prior academic performance had no impact on the medical school performance (2-tailed Pearson correlation 0.00). There was no positive correlation between the HSG, pre-clinical, and clinical GPA. 50% marks are dedicated to HSG which is not proved to be a reliable predictor of academic success in the medical schools. To overcome this shortcoming of HSG, semi structured interviews have been applied to have a holistic impression of the applicant’s performance and abilities. The interview component is supposed to assess the commitment and motivation to study medicine and communication skills. The assessment of communication skills covers four domains: comprehension, articulation, relevancy and interaction. In the semi structured interview, the element of bias cannot be ruled out and it is a time taking, tedious, and tedious task for the faculty members.
Conclusion
Selection in the medical schools is mainly based on HSG as a benchmark of prior academic performance. The present study found that HSG are poor predictors of academic performance of students in the medical school.
Limitations
The study is limited to the effect that previous academic performance was collected retrospectively and thus it was restricted to the information available in student files. Also the data from 2 groups (2005-2006) were available for complete analysis. Small sample size might not reflect a holistic view of the medical course.
Conflict of interest
The authors declare no conflict of interest and no competing intentions.
Acknowledgement
The authors highly appreciate the secretarial staff of the Vice Dean of Academic Affairs CMTU in providing the required data for the research.
References
- Baron J, Norman MF. SATs Achievement Tests, and High-School Class Rank as Predictors of College Performance. Educational and Psychological Measurement. 1992;52:1047-.
- James D, Ferguson E, Powis D, Symonds I, Yates J. Graduate entry to medicine: widening academic and socio‐demographic access. Medical education. 2008;42(3):294-300.
- Mercer A, Puddey IB. Admission selection criteria as predictors of outcomes in an undergraduate medical course: A prospective study. Medical Teacher. 2011;33(12):997-1004.
- Carter YH, Peile E. Graduate entry medicine: high aspirations at birth. Clinical Medicine, Journal of the Royal College of Physicians. 2007;7(2):143-7.
- Al-Rukban MO, Munshi FM, Abdulghani HM, Al-Hoqail I. The ability of the pre-admission criteria to predict performance in a Saudi medical school. Saudi medical journal. 2010;31(5):560-4.
- Pandey AS, Dixit HM. Selection criteria and pre-clinical academic performance in a private medical college in Nepal: A case study. Medical Teacher. 2011;33(4):186-92.
- van Niekerk DV, Christensen L, Karle H, Lindgren S, Nystrup J. WFME Global standards in medical education: Status and perspectives following the 2003 WFME World conference. Medical education. 2003;37(11):1050-4.
- McManus I, Smithers E, Partridge P, Keeling A, Fleming PR. A levels and intelligence as predictors of medical careers in UK doctors: 20 year prospective study. BMJ. 2003;327(7407):139-42.
- Haldane T, Shehmar M, Macdougall CF, Price-Forbes A, Fraser I, Petersen S, et al. Predicting success in graduate entry medical students undertaking a graduate entry medical program. Medical Teacher. 2012;34(8):659-64.
- Lumb AB, Vail A. Comparison of academic, application form and social factors in predicting early performance on the medical course. Medical education. 2004;38(9):1002-5.
- Halpern N. The impact of attendance and student characteristics on academic achievement: Findings from an undergraduate business management module. Journal of Further and Higher Education. 2007;31(4):335-49.
- Smith R. Why are doctors so unhappy? BMJ. 2001;322(7294):1073-4.
- Craig P, Gordon J, Clark R, Langendyk V. Prior academic background and student performance in assessment in a graduate entry programme. Medical education. 2004;38(11):1164-8.
- Wilkinson D, Zhang J, Byrne GJ, Luke H, Ozolins IZ, Parker MH, et al. Medical school selection criteria and the prediction of academic performance. Medical Journal of Australia. 2008;189(4):235.
- Ferguson E, James D, Madeley L. Factors associated with success in medical school: systematic review of the literature. BMJ. 2002;324(7343):952.
- Julian ER. Validity of the Medical College Admission Test for predicting medical school performance. Academic Medicine. 2005;80(10):910.
- Donnon T, Paolucci EO, Violato C. The predictive validity of the MCAT for medical school performance and medical board licensing examinations: a meta-analysis of the published research. Academic Medicine. 2007;82(1):100-6.
- Albanese MA, Snow MH, Skochelak SE, Huggett KN, Farrell PM. Assessing personal qualities in medical school admissions. Academic Medicine. 2003;78(3):313-21.
- Brotherton SE, Simon FA, Etzel SI. US graduate medical education, 2001-2002. JAMA: the journal of the American Medical Association. 2002;288(9):1073-8.
- Birch ER, Miller PW. Tertiary Entrance Scores: can we do better? Education Research and Perspectives. 2007;34(2):1.

