
Manuscript accepted on :March 20, 2009
Published online on: 12-11-2015
Plagiarism Check: Yes
Nagulu Malothu*, Uday Kiran Veldandi¹, Nalini Yadala² and Rama Krishna Devarakonda¹
¹Department of Pharmacology and Clinical Pharmacy, University College of Pharmaceutical Sciences, Kakatiya University, Warangal - 506 009 India.
2Departemt of Medicine, Kakatiya Medical College, Warangal - 506 009 India.
Corresponding Author E-mail:nagoncology@gmail.com
Abstract
Objective Warangal district in Andhra Pradesh, southern India, records over many cancer cases each year. We aimed to describe the frequency, distribution, and assess quality of management and subsequent outcomes from cancer in one large hospital in the district. Methods We reviewed data of all patients admitted with different types of cancer to a district government hospital for the years 2003 to 2006. For these years, details of the particular cancer patients admitted and management were abstracted from the medical files. Findings During these four years, 1753 patients were admitted in the hospital with different types of cancer. More detailed data from the years 2003, 2004, 2005 and 2006 reveals that older people are more prone to any type of cancer. Incidence of cancer is more in females. Most common type of cancer in females is cervix cancer in this part of country [30%]. Women above 40 age are prone to breast and ovarian cancers [20%].The most common type of cancer in males is mouth cancer [25%]. Conclusion It is likely that these findings reflect the situation in many rural hospitals of the southern India region. Even without an increase in resources, there appear to be significant opportunities for reducing cancer incidence by better medical management and further development on the reduction of cancer.
Keywords
Pharmacoepidemiology; Cancer; Southern India
Download this article as:| Copy the following to cite this article: Malothu N, Veldandi U. K, Yadala N, Devarakonda R. K.Pharmacoepidemiology of Cancer in Southern India. Biomed. Pharmacol. J.2009;2(1) |
| Copy the following to cite this URL: Malothu N, Veldandi U. K, Yadala N, Devarakonda R. K.Pharmacoepidemiology of Cancer in Southern India. Biomed. Pharmacol. J.2009;2(1). Available from: http://biomedpharmajournal.org/?p=611 |
Introduction
Pharmacoepidemiology is described as a bridge science because it spans clinical pharmacology, drug utilization, and epidemiology [1]. Pharmacoepidemiology is the ‘‘study of the use and effects of drugs in large numbers of persons.’’[2, 3].Cancer epidemiology is the study of the incidence of cancer as a way to infer possible trends and causes. Modern epidemiological methods are closely linked to current concepts of disease and public health policy. Over the past 50 years, great efforts have been spent on gathering data across medical practice, hospital, provincial, state, and even country boundaries, as a way to study the interdependence of environmental and cultural factors on cancer incidence.
Cancer epidemiology must contend with problems of lead time bias and length time bias. Lead time bias is the concept that early diagnosis may artificially inflate the survival statistics of a cancer, without really improving the natural history of the disease. Length bias is the concept that slower growing, more indolent tumors are more likely to be diagnosed by screening tests, but improvements in diagnosing more cases of indolent cancer may not translate into better patient outcomes after the implementation of screening programs. A similar epidemiological concern is over diagnosis, the tendency of screening tests to diagnose diseases that may not actually impact the patient’s longevity. This problem especially applies to prostate cancer [4]
In some Western countries, such as the USA, [5] and the UK [6, 7] cancer is overtaking cardiovascular disease as the leading cause of death. In many Third world countries cancer incidence appears much lower, most likely because of the higher death rates due to infectious disease or injury. With the increased control over malaria and tuberculosis in some Third world countries, incidence of cancer is expected to rise; this is termed the epidemiologic transition in epidemiological terminology.
Cancer epidemiology closely mirrors risk factor spread in various countries. Hepatocellular carcinoma (liver cancer) is rare in the West but is the main cancer in China and neighbouring countries, most likely due to the endemic presence of hepatitis B and aflatoxin in that population. Similarly, with tobacco smoking becoming more common in various Third world countries, lung cancer incidence has increased in a parallel fashion.
India and the world have crossed over to the new millennium, not to speak of a new century. It is thus an appropriate time not just to look back at the past, but to reflect on our needs and desires for the future. The first is that of Clinical Epidemiology, which is an essential area for integrating the health sciences as well as a pointer to the future trends. The second is that of Clinical Pharmacology, which has suddenly caught the imagination of people after the new WTO agreement. The meeting point of these two fields is therefore bound to generate sparks and ultimately produce an offspring. This offspring is already well established in certain countries. Its name is ‘Pharmacoepidemiology’.
Epidemiology is the study of distribution and determinants of diseases in populations. During its progress forward, epidemiology has inculcated precise and strict methodologies for the study of diseases. The application of these methodologies for the study of the use of and the effects of drugs in large number of people is the discipline of Pharmacoepidemiology.
The past reports of epidemiological studies of cancer reveal that the major cause of death of poor people in India is oral as well as cervical cancer which made me take up the study of epidemiology of cancer in this part necessary.
Methods
To evaluate differences in risk between populations requires incidence rates, derived from population based cancer registries, which aim to record information on all new cases of cancer occurring in a defined population.
We collected and reviewed data of all patients admitted with any type of cancer to the Mahatma Gandhi Memorial (MGM) Hospital, a district level government hospital in the city and district of Warangal, for the years 2003 to 2006.
The MGM Hospital is a 550-bed hospital located in the northern Telangana region of Andhra Pradesh. It is the referral hospital for cancer patients from Warangal district, although some cancer patients come from outside the district (in this study, >92% of patients were from Warangal). Most patients presenting to other hospitals in the district are transferred to MGM Hospital. Total in-patient admissions to the hospital average about 300 per day with many patients (usually admitted with fever) discharged within one day.
After medical checkup in a casualty ward, cancer patients are admitted to the Oncology; cancer care unit, which contains 20 beds and is staffed by four doctors and four nurses. Patients requiring radiation therapy are referred to the four-bedded Radiology intensive care unit, which has two doctors and two nurses.
Data were collected retrospectively from medical files. Only patients who were hospitalized were included in the study. Patients with cancer were identified from specific codes recorded at the time of admission. For patients admitted during 2003, 2004 2005 and 2006, information regarding gender, age, type of cancer, medication, treatment and outcome was abstracted from the medical records onto a data sheet. The data from all case sheets were entered into a database to calculate descriptive statistics on 2003, 04, 05 & 2006 presentations.
Results and Discussion
India is a country with over a billion in population. Each individual in the country has at one time or the other taken a drug. In many instances, a person takes more than one drug, and that too for a period of time. Unlike the West, where drug usage is strictly prescription based, ‘over the counter’ drugs are freely available in India. This leads to misuse and its consequences. To complicate matters, the people of India utilize various systems of medicine in Allopathy, Homeopathy, Ayurveda, Siddha, etc. In such a scenario, the discipline of Pharmacoepidemiology promises to maintain a close watch over the use of drugs and their effects on people. If this monitoring and reviewing process is absent, the pharmacological effects of drugs, their adverse effects, interactions and misuse can play havoc with the health system in this country.
A few examples are needed to drive home the point. In the 1930’s, the marketing of elixir of sulphanilamide dissolved in diethylene glycol resulted in the death of over 100 children (1). In the 1960’s, pregnant ladies who ingested thalidomide gave birth to children with phocomelia. (2). In the 1970’s, practolol usage led to oculomucocutaneous syndrome (3). In the last two decades, many drugs have been withdrawn from the market
because of serious ADRs. In India though, inspite of the large volume of drugs being consumed, hardly any major problem with drugs have been recognized. Could that be due to the lack of pharmacoepidemiologists [8]
The sort of problems experienced by the world in drug usage will not disappear overnight. It will only increase as one sees from the huge array of new drugs entering the market. Thus the potential of pharmacoepidemiology for addressing these problems become clear
Geographical location, genetic makeup, culture, physical exercise etc. For example, in India mouth cancer is common in the regions where betel nut chewing, tobacco consumption in the form of chewing or smoking is prevalent. Reverse smokers are more at risk developing cancer of palate [9].
Epidemiological studies have shown that 70 to 90% of all cancers are due to environmental exposures. Life style related factors are the most important and preventable among the environmental exposures. Tobacco consumption either chewing or smoking accounts for 50% of all cancers in men. Dietary practices reproductive and sexual practices etc. account for 20 to 30% of cancers. Comparatively older people are more prone to cancers. Brain cancer and blood cancers are common in children. Men above 50yrs are prone to prostrate cancer while women above 45yrs are prone to breast, cervical and ovarian cancers [10].
This study reviews known causes of cancer and quantifies the proportion of the cancer burden in southern India that they explain. The quantities presented measure the changes in the occurrence of the disease that we would expect following the removal of those causes; in other words, the potential impact of primary prevention. Numbers of cases and deaths are attributed to broad categories of causal factors for use in public health planning. With the work presented the authors aim to providing a source of objective and quantitative information to help public health planners, administrators, service providers as well as the general public in their actions to prevent cancer. The study presents comprehensive data on cancer incidence for over south Indian populations. The time-period covered is 2003- 2006, making available information on patterns and trends of cancer for over 40 years for the older-established cancer registries.
Almost all patients were direct admissions to MGM Hospital; very few patients were transferred from small rural hospitals surrounding Warangal city. During 2003-2006, 1753 patients were admitted to the hospital with any type cancer [Table 1]. The most patients in one year were 607 in 2003 among them 156,138, 95 patients with cervix, mouth and breast cancers respectively. Brest cancer incidence was more and increased every year from 2003 to 2006.Cervix cancer incidence was decreased. [Fig 2]Women outnumbered Men with all cancer types (Fig 1). Two thirds of patients were aged in between 40-50 [Fig 3].
Table 1: Annual number of cancer patient admissions at the Mahatma Gandhi Memorial hospital (2003-2006).
|
Type of Cancer |
TOTAL NO OF PATIENTS [ YEAR ] | |||
| 2003 | 2004 | 2005 | 2006 | |
| Cervix | 156 | 111 | 70 | 60 |
| Mouth | 138 | 88 | 75 | 90 |
| Breast | 95 | 73 | 57 | 120 |
| Esophagus | 38 | 20 | 5 | 16 |
| Lung | 22 | 15 | 5 | 6 |
| Lymphomas | 21 | 34 | 4 | 10 |
| Stomach | 18 | 22 | 8 | 4 |
| Ovary | 16 | 7 | 8 | 5 |
| Colorectal | 15 | 15 | 3 | 5 |
| Brain | 10 | 15 | 3 | 6 |
| Liver | 9 | 10 | 3 | 7 |
| Penis /Testes | 9 | 12 | 4 | 2 |
| Thyroid | 7 | 10 | 4 | 3 |
| U-Bladder | 6 | 7 | 0 | 1 |
| Pancreas | 6 | 3 | 0 | 0 |
| Others | 41 | 52 | 43 | 25 |
| TOTAL | 607 | 494 | 292 | 360 |
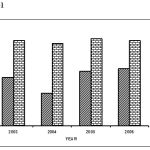 |
Figure 1: Percentage of Male and female cancer patients (2003-2006).
|
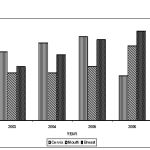 |
Figure 2: Percentage of cervix, Breast and Mouth cancer incidence (2003-06).
|
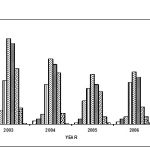 |
Figure 3: Cancer incidences in different age intervals during the years 2003-2006.
|
Treatment in breast cancer
There are four stages in breast cancer. Treatment approach depends on type of stage of cancer. Stage I, II, and IIIA require surgery followed by adjuvant treatment with radiotherapy or chemotherapy or hormonal therapy or combination of two depending on the IHC marker study. IIIB stage requires chemotherapy followed by surgery and radiotherapy and IVA stage requires systemic therapy with drugs like hormones, 5-Flourouracil, Methotrexate, Cyclophospamide & Doxorubicin along with supportive therapy is effective. Breast conservation therapy with lumpectomy for small tumors is possible now with limited surgery, post operative radiotherapy and Chemotherapy. This option is proffered by younger patients.
Treatment in oral cancer
In early period oral malignancy occurs in two stages i.e. T1 and T2. In both T1 and T2 stages either surgery or radiotherapy is effective. In advanced stage combination of surgery and radiotherapy is required. Radiotherapy is either prior to surgery or after surgery depending on the stage and nature of cancer. In oral, laryngeal and hypo laryngeal cancer the latest protocol is organ preservation, in which the patient is subjected to concomitant chemo irradiation. i.e. combination of radiation and chemotherapy with 5-Flourouracil and cisplatin.
Treatment in cervical cancer
There are four stages in cervical cancer i.e. stage Ia, Ib, IIa, IIb, IIIa. IIIb, IVa and IVb. In stage Ia, Ib and IIa surgery or radiotherapy results are equal. Concomitant chemo irradiation is current choice of treatment In more than stage IIb desease. Chemo irradiation for bulky tumors (having more than 4 cm in size) includes single agent cisplatin along with radiotherapy. In stage IVa and IVb radiotherapy is effective for palliation.
This study has been carried out in Oncology department MGM Hospital Warangal which caters to neighbouring districts like Nalgonda, Khammam,Karimnagar, Adilabad and Rangareddy.1753 patients were registered from january 2003 to Dec 2006.
Conclusions
From this study
It is found that older people are more prone to any type of cancer.
Incidence of cancer is more in females. Most common type of cancer in females is cervix cancer in this part of country. It accounts for 30%.
Women above 40 age are prone to breast and ovarian cancers. It accounts for 20%.
The most common type of cancer in males is mouth cancer. It accounts for 25%.
Reference
- Notes from the guest editors, Pharmacoepidemiology – a bridge science; Norwegian Journal of Epidemiology, 11 (1): 3-4(2001).
- Strom,B.L.,Tugwell,P, .Pharmacoepidemiology: current status, prospects, and problems. Ann Intern Med. 113:179-81(1990).
- EsmondD,N., Karen,L.R.,Leticia,R.M and James,P.W, harmacoepidemiology Education in US Colleges and Schools of Pharmacy; American Journal of Pharmaceutical Education, 71 (4) Article 80(2005).
- Brawley,O.W, .Prostate cancer screening: clinical applications and challenges.Urol. Oncol ,22 (4): 353–7(2004).
- Jemal,A., Murray,T., Ward,E., Samuels,A. ,Tiwari,R.C., Ghafoor,A., Feuer,E.J and Thun,M.J,Cancer statistics. CA Cancer J Clin ,55 (1): 10–30 (2005).
- National Cancer Institute Questions and Answers About Beta Carotene Chemoprevention Trials U.S. National Institutes of Health
- Cancer: Number one killer . BBC News online. Retrieved 2005-01-29(2000).
- Himanshu,S., Mohammed,A ., Faisal,I ., Mohammad,SA.,Prem ,K and Krishna,K.A, pharmacovigilance study in the department of medicine of a university teaching hospital. Pharmacy Practice (Internet) ISSN 1886-3655 version on-line.
- Lee PN .Smoking “attributable” mortality in India Some relevant considerations ; (1996)
- Roger,Z.,Anderson,R.,Cefalu,C and Sidani,M, Cancer screening guidelines.American Family Physician, 63( 6):20-23 (2001).

