
Manuscript accepted on :24-Aug-2018
Published online on: 06-09-2018
Plagiarism Check: Yes
Reviewed by: Burak Buldur
Second Review by: Mandeep Kaur
Final Approval by: Dr. H Fai Poon
Pavithra H. Dave1, Deepa Gurunathan2 and Madhu Sudhan Vasantharajan2
1Saveetha Dental College, Saveetha University, Chennai, India.
2Department of Pedodontics Saveetha Dental College, Saveetha University, Chennai, India.
Corresponding Author E-mail: drgdeepa@yahoo.co.in
DOI : https://dx.doi.org/10.13005/bpj/1509
Abstract
Pediatric syrup formulations have been used for a long time in medicine. Cough syrups and other liquid medications are available easily and widely accepted by the children. The high intake of oral medications can be the causative factor for dental erosion and decay. Hence the aim of this study is to compare the efficacy in the pH levels of the saliva before and after the consumption of cough syrups. The study included 50 volunteer children. Children were recruited from the general medicine ward at Saveetha Medical College and Hospitals. Criteria for inclusion are candidates to be completely recovered within 5 days from upper respiratory tract infections such as common cold, cough and asthma. Children not recovering for more than 5 days and with other bacterial infections such as pneumonia, tuberculosis and other chronic respiratory ailments were excluded from the study. Prior to the study, its essence was explained to participants and their parents so that they could provide an informed consent. The collected data were analysed with IBM.SPSS statistics software version 23.0 (2009) to describe about the data descriptive statistics frequency analysis. To find the significant difference between the bivariate samples in Paired groups the Paired sample t-test was used. The pH levels before the consumption of cough syrups was found to be 7.09 and after consumption was 6.86 and the significant p value was calculated to be 0.0002 thus being statistically significant. The present study finds a significant drop in salivary pH level following the intake of cough syrup, which makes them a risk factor for the development of dental caries, and especially in childhood.
Keywords
Cariogenic Potential; Cough Syrup; Flow Rate; pH; Saliva
Download this article as:| Copy the following to cite this article: Dave P. H, Gurunathan D, Vasantharajan M. S. Comparison of pH Levels of the Saliva Before and After the Consumption of Cough Syrups in Children. Biomed Pharmacol J 2018;11(3). |
| Copy the following to cite this URL: Dave P. H, Gurunathan D, Vasantharajan M. S. Comparison of pH Levels of the Saliva Before and After the Consumption of Cough Syrups in Children. Biomed Pharmacol J 2018;11(3). Available from: http://biomedpharmajournal.org/?p=22272 |
Introduction
Pediatric syrup formulations have been used for a long time in medicine. Cough syrups and other liquid medications are available easily and widely accepted by the children. The high intake of oral medications can be the causative factor for dental erosion and decay. The sugars may not be present only in biscuits and chocolates but may also be present in these oral formulations.1
These liquid medicines contain acidic agents along with sweetners which act as buffers for maintaining the stability, tonicity and for ensuring physiological compatibility.2 The acid production is enhanced when the carbohydrates are in contact with the oral cavity. The dissolution of carbohydrates such as sucrose contributes to the formation of caries.
So the rate of salivary clearance is one of the determining factors for the availability of fermentable substrates to the bacteria.3 Regular use of sugar-containing liquid medicines is often the cause of dental caries in children.
Children on an average take medicine every eight hours daily or 10 times a week. Moreover, other healthy children who take medicines infrequently and for short periods are also at risk of development of dental caries.4 The risk factors for increased level of caries are liquid medications taken for duration of three months or more and the most affected region being the posterior teeth than anterior teeth.5
Taken at night they can be an aggravating condition, because during this period salivary flow rate is reduced and the time of elimination from the oral cavity rises.6
A major role is played by saliva in modifying plaque pH, especially in caries-resistant people.7 Saliva acts as a major modulating factor to maintain hemostasis. Records show that is great variation in individual salivary flow rates and in its ionic compositions.8 Majority of the pediatric liquid medicaments used in the study are acidic in nature with pH below 7 and the pediatric liquid medicaments frequently used have erosive effect on enamel of deciduous teeth.9 The cariogenic potential of most commonly prescribed liquid oral medicines for children depends on the percentage of sugar concentration and pH of these medicines.10
The Stephan Curve has played a dominant role in caries research over the past several decades. Stephan Curve illustrates the plethora of interactions and yet acid production remains the dominant focus.11 Hence this study aims to compare the pH levels in the saliva before and after the consumption of cough syrups.
Materials and Methods
This was an in vivo comparative study and was initiated after approval from Institutional Ethical Review Board of Saveetha Dental College and Hospitals, Chennai. The present study consisted of comparing the pH levels before and after the consumption of cough syrups. Lack of previous studies done on effect of cough syrups on saliavry pH, prompted us to do this study.
Prior to the clinical examination its essence was explained to participants and their parents so that they could provide an informed consent.Verbal and written consent was obtained from the participants of the study.
The study consisted of three syrups: Three most commonly available over-the-counter drugs were randomly selected. These randomly chosen drugs belonged to different pharmaceutical manufacturing units- CHERICOF(Ranbaxy) which is a combination of phenylephrine and dextromethorphan, CODISTAR(mankind pharma) which is a combination of dextromethorphan and chlorpheniramine maleate and COLDREX(omega pharma) which contains dextromethorphan and promethazine. The literatures and the labels on these bottles were also collected so as to gather any information necessary for the study. Allotment of the selected subjects to a particular group was made by lottery system.
Study setting: The study included 50 volunteer children. This study was conducted for a period of three months from November 2017 to January 2018. Children in the age group 6 to 12 years who visited the general medicine ward at Saveetha Medical College and Hospitals were recruited for the study.
Inclusion and Exclusion Criteria: Criteria for inclusion are candidates who are under medications for any upper respiratory tract infections such as common cold, cough and asthma. Children not recovering for more than 5 days and with other bacterial infections such as pneumonia, tuberculosis and other chronic respiratory ailments were excluded from the study.
Collection of saliva samples: The study was done in the morning with standard oral hygiene habits. The unstimulated saliva is tested. The volunteers provided 1-2 spit samples in a sample cup (figure 1). During the course of the study, saliva pH was measured at the appropriate time intervals with medication intake. Thus, the saliva pH values serving as baseline control. Following the cessation of the cough syrups the subsequent saliva samples were taken and data was tabulated. The data was entered in a Performa sheet using the Microsoft Excel Version 12.0(2007) software.
pH measurement: The pH of all the drugs was determined using digital pH meter with glass combination electrode, which was previously calibrated with pH 7 and pH 4 buffer solutions. An in-vitro Saliva Check test is applied with pH meter that shows the pH level on the LED screen (figure 2).
The pH meter was standardized in a buffer solution containing hydrochloric acid and sodium hydroxide solution and was calibrated (figure 2).
Statistical analysis: A paired T test analysis is performed to verify the differences in the values and statistical analysis was completed. The collected data were analysed with IBM.SPSS statistics software 23.0 Version (2009). To find the significant difference between the bivariate samples in Paired groups the Paired sample t-test was used.
Based on the knowledge of the saliva buffer capacity and the quick drop in pH below the critical values after intake of simple carbohydrates and its slow rise to baseline, requiring 15 to 40 minutes (demonstrated by the Stefan curve).
 |
Figure 1: Collected Saliva Samples.
|
Figure 1. Depicts the saliva sample collected in sterile containers both before and after the consumption of cough syrups.
 |
Figure 2: pH Meter Indicating the Levels.
|
Figure 2. depicts pH meter that shows the pH level on the LED screen.
Results
The collected data were analysed with IBM.SPSS statistics software 23.0 Version (2009).To describe about the data descriptive statistics frequency analysis, percentage analysis were used for categorical variables and the mean & S.D were used for continuous variables. To find the significant difference between the bivariate samples in Paired groups the Paired sample t-test was used. In the above statistical tool the probability value .05 is considered as significant level.
Table 1: Paired Samples Statistics.
| Mean | N | Std. Deviation | Std. Error Mean | |
| pH of saliva before taking cough syrup | 7.0860 | 50 | .23561 | .03332 |
| pH of saliva after taking cough syrup | 6.8600 | 50 | .38439 | .05436 |
Table 1. depicts the paired sample statistics before and after the consumption of cough syrup.
Table 2: Paired Samples Test.
| Mean | Std. Deviation | t | Significance (p) | |
| pH of saliva | 0.226 | 0.39217 | 4.075 | 0.0002 |
Table 2. depicts the paired sample test which gives a p value= 0.0002 thus being statistically significant.
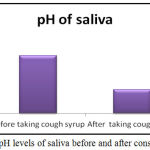 |
Figure 3: pH levels of saliva before and after consumption.
|
Figure 3. depicts the chart of the salivary pH levels before and after the intake of cough syrups. The levels before the consumption were 7.09 and after consumption were 6.86.
Discussion
Saliva plays a critical role in maintaining oral homeostasis; it modulates the ecosystem through lubrication of the alimentary bolus, protection against microorganisms, buffer and repair of the oral mucos a, and helps in dental remineralization.11 Unstimulated whole saliva that reflects basal salivary flow rate is present in our mouths for about 14 hours a day and is the secretion that provides protection to oral tissues. Stimulated saliva represents the secretion during food intake (physiologic stimulation) and is present in the oral cavity for up to 2 hours.12
The use of different types of conventional medications in childhood is widespread. The characteristics determining the medication caries prone potential are the sucrose content, the acidic nature of the drug and the individual salivation and salivary buffer capacity.13 The cariogenic potential of pediatric liquid drugs is due to the high concentration of fermentable carbohydrates and their acidity. 5% sucrose solution concentration is considered sufficient to form a cariogenic biofilm. Citric acid is the most commonly used primary acid in the oral medicines, though being a weak acid, it is a potent erosive agent. It has also been reported that as the pH decreases, the potential of enamel erosion increases.14
In a study by Pradhan et al it is concluded that the drop in salivary pH below the critical values takes place up to 6 minutes after rinsing with a 25% sucrose solution, making children taking sucrose medications prone to caries. As Bigeard et al claim, the increasing intake of prescripted drugs and the self-medication in developed countries puts a growing number of children at a risk of drug-related caries, which can be considered a public health problem.15
The fall in the pH causes incidences of tooth decay to occur which is also aggrevated by factors such as acidic food and drinks thus contributing to dental caries. Stephan Curve shows the change in the pH of dental plaque in response to a 10% sucrose solution. A rapid drop in pH is recorded followed by a slow rise until the pH returns to the normal resting value. This means that patients suffering from xerostomia (dry mouth) are more susceptible to dental caries. When attempting to reduce caries, the individual diet should be examined and this is best achieved through dietary analysis through the use of a diet sheet.16
The use of cough syrups is effective, relatively inexpensive, and patients are satisfied and rarely experience side effects. The convenient form of this type of medication and its sweet and pleasant taste and smell make it suitable and well-received among children. There are still some rules that need to be followed by the administration of these medicines. They are prescribed with frequent intake – usually 3-4 times a day, and sometimes every two hours, on a regular basis and at night before bedtime.17 According to our results this will cause a drop in saliva pH and maintenance of a long-lasting acidity over a long period of time. The later is further aggravated by the fact that the intake of a medication should be at least 15 minutes before or after meals. During the treatment pastes without sweeteners, synthetic deodorants, bleaching agents, artificial colors or fragrances, detergents, mint should be also used. The pastes should not contain fluorides.18
The sugars present in the cough syrups can also affect the oral health of the children and be at a higher risk of developing caries from an early age.19
The daily use of medications for most children is usually for a short time, but for some, it could be over a prolonged period. The long‑term use of prescribed medicines by chronically ill children is known to cause dental caries. A survey of pediatric liquid medicines in New Zealand revealed that over half of prescribed and over‑the‑counter medicines for children contain sugar. It has been shown that continuous administration of sucrose‑based medicines causes dental caries and related gingivitis.20
Therefore depending on their composition, frequency of application, and length of therapy, the oral health of children undergoing treatment should be monitored. This fact we attribute to its high sucrose content, its low viscosity, and its acidic endogenous pH.
Conclusion
The current study concludes that the salivary pH levels did not return to baseline values following one hour of administration of cough syrups. This, along with the specific rules for the intake of medications and their use in patient own discretion without prescription, makes them a risk factor for the development of dental caries, especially in childhood. Healthcare professionals and parents should apply prophylactic measures while using cough syrups.
References
- Nankar M. Comparative evaluation of cariogenic and erosive potential of commonly prescribed pediatric liquid medicaments: an in vitro study. The journal of contemporary dental practice. 2014;15(1):20.
CrossRef - Pradhan D. Effect of the presence of dental plaque on oral sugar clearance and salivary pH: an in vivo study. J Contemp Dent Pract. 2012;13(6):753-755.
CrossRef - Saeed S. An in vitro analysis of the cariogenic and erosive potential of pediatric liquid analgesics. Journal of Indian Society of Pedodontics and Preventive Dentistry. 2015;33(2): 143.
CrossRef - P. B .S and Raju O. A comparison of oral hygiene status and dental caries in children on long term liquid oral medications to those not administered with such medications. J Indian Soc Pedo Prev Dent. 2002;20(4):144-151.
- Pomarico L., Souza I and Tura L. R. Sweetened medicines and hospitalization: caries risk factors in children with and without special needs. European Journal of Paediatric Dentistry. 2005;6(4).
- Abelson D and Mandel I. The effect of saliva on plaque pH in vivo. Journal of dental research. 60(9):1634-1638.
CrossRef - Wu K.P. Relationship between unstimulated salivary flow rate and saliva composition of healthy children in Taiwan. Chang Gung Med J. 2008;31(3):281-6.
- Mittal S. Surface changes of primary tooth enamel by commonly used pediatric liquid medicaments: A scanning electron microscope study. Journal of Pediatric Dentistry. 2017;5(1):14.
CrossRef - Agrawal N. Cariogenic potential of most commonly prescribed liquid oral medicines for children.
- Saravanan S. Prevalence pattern of dental caries in the primary dentition among school children. Indian Journal of Dental Research. 2005;16(4).
CrossRef - Zhao D. Paediatric Over-the-Counter (OTC) Oral Liquids Can Soften and Erode Enamel. Dentistry Journal. 2017;5(2).
- Deepa T and Thirrunavukkarasu N. Saliva as a potential diagnostic tool. Indian journal of medical sciences. 2010;64(7).
CrossRef - Dhivyalakshmi M and Maheswari T. U. Expression of salivary biomarkers–Alkaline phosphatase & lactate dehydrogenase in oral leukoplakia. Int J Chemtech Res. 2014;6:3014-18.
- Hahnemann S., Reily O. W. B. editor. Organon of the Medical Art. Palo Alto, California (USA): Birdcage Books. 1996.
- Valinoti A. C., da Silva., Pierro V. S., da Silva E. M., Maia L. C. In vitro alterations in dental enamel exposed to acids medicines. International Journal of Paediatric Dentistry 2011;21:141-150.
CrossRef - Sahgal J., Sood P. B., Raju O. S. A comparison of oral hygiene status and dental caries in children on long term liquid oral medications to those not administered with such medications. J Indian Soc Pedod Prev Dent. 2002;20:144–151.
- Rekola M. In vivo acid production from medicines in syrup form. Caries Res 1989;23:412‑6.
CrossRef - Nirmala S. V. S. G., Popuri V. D., Chilamakuri S., Nuvvula S., Veluru S., Babu M.S. Oral health concerns with sweetened medicaments: Pediatricians. J IntSoc Prevent Communit Dent. 2015;5:35-9.
CrossRef - Dunning J. M. Epidemiology: Dental caries. Principles of Dental Public Health. 4th edn. Cambridge. 1986.
- Finn S. B. Clinical Pedodontics. 4th edn. Philadephia W. B. Saunders Company. 1991;454-474.

