
Manuscript accepted on :May 30, 2017
Published online on: --
Plagiarism Check: Yes
Alexey L. Charyshkin1, Alexander A. Maxine2, Maxim V. Yashkov1, Lyubov V. Matveeva1 and Alexander V. Poteryaev2
1Department of surgery, Ulyanovsk State University 432017, Leo Tolstoy Str, 42, Ulyanovsk, Russian Federation.
2GUZ "Ulyanovsk Regional Clinical Hospital” 432017, Third International Str., 7 Ulyanovsk, Russian Federation.
Correspoding Author E-mail: AlexeyCharyshkin@yandex.ru
DOI : https://dx.doi.org/10.13005/bpj/1189
Abstract
A clinical case of the use of distal reconstructive vascular operations in a patient with critical ischemia of the lower limb is presented in the article. A high-risk patient with multifocal atherosclerosis suffered a bifurcational aorto-femoral shunting in 2005, an acute myocardial infarction, suffers from ischemic heart disease, exertional angina of 3 FC. After 10 years after the operation, he began to note the deterioration. Semi-closed loop endarterectomy from the right SFA and direct endarterectomy from the mouth of the right DFA was performed at the first stage. On the next stage a semi-closed loop endarterectomy from the RCA on the right and a direct endarterectomy from the mouth of ATA, PTA were performed. Was performed an overlapping of AV fistula between ATA and ATV, popliteal pedidial shunting below the knee cleft between RCA and ATA. After 43 bed days, after the stage of reconstructive vascular surgeries on the right foot by Chopar’s amputation. After 4 months, was performed the dermepenthesis of the post-surgery stump. Was examined in March 2017, the patient's condition is satisfactory. The clinical case shows that distal combined reconstructive vascular surgeries can save limbs in patients with critical ischemia of the lower limb and multifocal atherosclerosis.
Keywords
Multifocal atherosclerosis; critical ischemia of the lower limb; reconstructive vascular surgery; endarterectomy
Download this article as:| Copy the following to cite this article: Charyshkin A. L, Maxine A. A, Yashkov M. V, Matveeva L. V, Poteryaev A V. Reconstructive Vascular Surgeries in A Patient With Critical Ischemia of the Lower Limb and Multifocal Atherosclerosis. Biomed Pharmacol J 2017;10(2). |
| Copy the following to cite this URL: Charyshkin A. L, Maxine A. A, Yashkov M. V, Matveeva L. V, Poteryaev A V. Reconstructive Vascular Surgeries in A Patient With Critical Ischemia of the Lower Limb and Multifocal Atherosclerosis. Biomed Pharmacol J 2017;10(2). Available from: http://biomedpharmajournal.org/?p=15413 |
Introduction
At present, the number of patients with multifocal atherosclerosis and critical ischemia of the lower extremities in the Russian Federation has increased. This is due to the increase of elderly and senile persons among the population [1, 5, 6, 7, 8].
According to the literature, critical ischemia of the lower extremities complicates the course of obliterating atherosclerosis in 33% of patients [5, 9, 10, 11]. Annually 1 in 100 patients with intermittent claudication passes into the group of patients with critical limb ischemia [12]. As a result of reconstructive interventions on the vascular bed in patients with critical ischemia of the lower extremities, the lethality reaches 14.0%, the number of amputations is 20.4% [4, 5, 6, 12]. Reconstructive surgical interventions provide preservation of the limb in the postoperative period up to 5 years to 80% of patients, and only to 50% after 10 years [2, 3, 4, 5, 6]. In some cases, distal combined reconstructive vascular surgeries help to save patient’s limb.
The man is 64 years old, on the 27.07.2015 enrolled in the thoracic department of the State Healthcare Institution of Ulianovsk Regional Clinical Hospital with complaints of pain in the right foot at rest, trophic ulcer on the right foot, intermittent claudication in the right anticnemion after 10-20m and in the left anticnemion after 300m. Anamnesis morbi: in 2005 the patient underwent a bifurcational aorto-femoral shunting. In the year 2005 he has suffered an acute myocardial infarction. He suffers from ischemic heart disease, angina pectoris of 3 FC. After 10 years after the operation, he began to notice a deterioration: there were pains in the lower limbs when walking, a trophic disorder on the right foot.
Status localis on admission: the feet are cool, the right is colder than the left. Pulsation on the arteries of the lower extremities on the right and on the left: on the femoral arteries distinct, distal (on the popliteal, back arteries of the feet) is not determined. Arterial pulsation on carotid arteries and arteries of the upper limbs is satisfactory. Movement and sensitivity in l/l and u/l are preserved in full. At the rear of the right foot, an oval-shaped trophic ulcer is covered with a necrotic scab of 8×5 cm (Fig. 1).
 |
Figure 1: Trophic ulcer of the dorsum surface of the right foot. |
According to the data of ultrasound duplex scanning of the arteries of the lower extremities conducted on 24.07.2015, the occlusion of both superficial femoral arteries, collateral blood flow in both popliteal arteries is preserved, in the arteries of the shin on the right – the collateral blood flow and the collateral blood flow in the left posterior tibial artery are preserved and the occlusion of the left anterior tibial artery in the upper third.
According to echocardiography from 27.07.15 a slight hypokinesia of the apex and interventricular septum.
According to the aortic arteriography of the lower extremities from 31.07.15 the right prosthesis’ jaw is anastomosed with the common femoral artery. The right superficial femoral artery is occluded from the mouth to the c/3 of the thigh. The right popliteal artery is occluded at the level of bifurcation. Right ATA (anterior tibial artery) contrasts with the middle third. Right PTA (posterior tibial artery) is stenosed along the entire length (Photo 2, 3, 4).
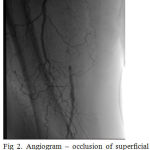 |
Figure 2: Angiogram – popliteal-pedidial segment.
|
 |
Figure 3: Angiogram – occlusion of superficial femoral artery. |
 |
Figure 4: Angiogram – popliteal-pedidial segment.
|
Indications for surgical treatment: Given the localization of the arterial involvement of the right lower extremity, the first stage of the surgery was performed on 04.08.15: semi-closed loop endarterectomy from the right SFA (surface femoral artery) with the help of the Wolmar’s ring, direct endarterectomy from the mouth of right DFA (deep femoral artery). Fibrotic AP (atherosclerotic plaque) up to 25 cm long was removed from the SFA during the operation. A satisfactory antegrade and retrograde blood flow was obtained, after restoration of the integrity of the vascular wall, a distinct ripple is higher and lower than the anastomosis. The operation is completed by draining the postoperative wound. On the 1st day (05.08.15) after the operation, arterial pulsation is determined only on the common femoral artery on the right and on the popliteal artery, however, limb ischemia is not stopped. It was decided to perform a revascularization of the peripheral arterial bed of the right lower limb. The next stage on 21.08.15: was performed a semi-closed loop endarterectomy from the PA (popliteal artery) on the right, direct endarterectomy from the mouth of ATA, PTA. Overlapping of AV fistula between ATA and ATV (anterior tibial vein). Popliteal-pedidial shunting is below the knee cleft between PA and ATA. Access is made along the Ken’s line in the upper third of the shin, along the medial surface. The distal part of PA, ATA, PTA, are on sutures. The arteries are tight to the touch, pulsation is not determined. Systemic heparinization is 5000 units endovenously. The PA is longitudinally dissected above the level of bifurcation. Retrograde blood flow from the pedidial arteries is weak. A direct endarterectomy was performed from the mouth of ATA, PTA – the blood flow increased. The Fogarty catheter 3f went in a distal direction: 3 cm in ATA and 1 cm in PTA. A semi-closed looped endarterectomy from PA with the help of the Wolmar’s ring was conducted, 8 cm fibrotic AP was removed, the remains of AP were removed with the help of a Fogarty catheter 5f, pulsating main blood flow was obtained. Access is made in the middle third of the right shin along the outer surface. Marked ATA, ATV. ATA is tight to the touch, pulsation is not determined. Arterial lumen is opened, the retrograde blood flow is very weak. The Fogarty catheter 3f passed in a distal direction for 15cm. Through the individual incisions on the hip, the trunk of the GSV was marked for 20 cm, the inflows were bandaged. The vein was washed with saline solution with heparin, reversed, dilated, prepared for the application of anastomosis. An oblique anastomosis was placed along the end-to-side type between the autovenous and distal part of the PA using a 6/0 prolene thread on the atraumatic needle. After the removal of vascular clamps, pulsation was below the level of anastamosis. Systemic heparinization is 2500 units of heparin endovenously. A tunnel is formed through the interosseous membrane. Autovein was put in the area of the lateral wound. An oblique anastomosis was placed between the autovein and ATA in the middle third with the formation of AV fistula (arterio-venous fistula) between ATA and ATV with the 7/08 “prolene” thread (Photo 5, 6). After removal of the vascular clamps, a distinct pulsation is lower than the anastomosis, systolic-diastolic tremor in the ATV.
 |
Figure 5: Access to PA, an anastomosis is imposeapplied between PA and autovein.
|
 |
Figure 6: Access to ATA of right l/l Anastomosis between autovein and ATA was applied with the formation of AV-fistula between ATA and ATV.
|
According to the results of the postoperative duplex sonography of the arteries of the right l/extremity from 21.08.15 the blood flow through the popliteal – pedidial shunt is magistral, the area of the anastomosis is passable. On the right ATA blood flow is magistrally-changed, speed is 131.0 cm/sec. On the right PTA, the blood flow is collateral, the velocity is 33.0 cm/sec. In the veins, blood flow is with arterial features.
The presence of necrotically altered tissues on the back surface of the right foot without a tendency to decrease and scarring within 42 days, as well as the presence of degenerative changes in the bones of the right foot, confirmed radiographically on 31.08.15, is an indication for surgery: Chopar’s amputation of the right foot. This surgical intervention was performed after 43 bed days, after the stage of reconstructive vascular surgeries.
On the 13th day after Chopar’s amputation of the right foot, we could see necrotic tissue at the edges of the flap, which served as an indication for performing necretomy and applying secondary sutures to the post-amputation stump.
The patient was dismissed after 3.5 months from the date of hospitalization with improvement. The patient managed to retain the limb. After 4 months, was performed the dermepenthesis of the postoperative stump. Later, the skin flap adequately took root. Examined in March 2017 (at the time of writing the article): the patient’s condition is satisfactory. Blood flow through the formed popliteal-pedidial shunt is adequate from 24.03.17. The phenomenon of critical limb ischemia did not occur (Photo 7).
 |
Figure 7: Right lower limb, condition after combined treatment.
|
Critical limb ischemia, causing severe disruption of vital functions, including statodynamic ones, is a direct source of social loss. Reconstructive vascular surgeries can completely or almost completely stop the signs of arterial insufficiency. [12]. According to the literature, the most severe social losses occur after amputation of thigh and lower leg [12]. With distal amputations, the patients’ appeal for prosthetic and orthopedic care is higher than with amputations at the hip level. In this connection, vascular surgeons face an important social and economic task of preserving limbs affected by critical ischemia by way of adequate revascularization.
Acknowledgment
The study was conducted with the financial support of the Ministry of Education and Science of the Russian Federation in the framework of the state support of the scientific project No. 18.7236.2017/БЧ.
References
- Abalmasov K.G., Buziashvili Yu.I., Morozov K.M. 2004. Quality of life of patients with chronic ischemia of lower extremities. Angiology and Vascular Surgery, 10(2): 8–13.
- Gavrilenko A.V. 2001. Evaluation of quality of life of patients with critical ischemia of lower extremities. Angiology and Cardiovascular Surgery, 2001. 3: 8–14.
- Galstyan G.Ye. Algorithm for diagnosis and treatment of arterial diseases of the lower extremities. Consilium Medicum, 2006. 8(12): 34–38.
- Ismailov N.B., Semenenko D.S. Vesnin A.V. The results of surgical treatment of gerontological patients with chronic ischemia of the lower extremities. In: Gerontology and geriatrics, Moscow, Vol. 7. 2007. pp. 256–260.
- Katelnitsky I.I. Opportunities of operative treatment of geriatric patients with critical ischemia of the lower extremities. Successes of Gerontology, 2012. 25(3): 338-342.
- Shevchenko Yu.L. Medico-biological and physiological basis of cellular technologies in cardiovascular surgery. Saint Petersburg, Science. 2006.
- Dominguez L.J., Barbagallo M., Sowers J.R., Resnick L.M. Magnesium responsiveness to insulin and insulin-like growth factor I in erythrocytes from normotensive and hypertensive subjects. Journal of Clinical Endocrinology and Metabolism, 12. 1998: 4402–4407.
CrossRef - Ruth S. Dilemma of Angiogenesis. Circulation, 2000. 10: 23.
- Rutherford R.B., Baker J.D., Ernst С. Recommended standards for reports dealing with lower extremity ischemia: Revised version. Journal of Vascular Surgery, 1997. 26: 516–538.
- Sandberg T. Paracrine stimulation of capillary cell migration tissue involves epidermal growth factor and is mediated via urokinase plasminogen activator receptor. Journal of Clinical Endocrinology and Metabolism, 2001. 86(4): 1724–1730.
CrossRef - Shintani S. Augmentation of postnatal neovascularization with autologous bone marrow transplantation. S. Shintani Circ., 2001. 103: 895–897.
CrossRef - Zoloyev G.K. Obliterating arterial diseases. Surgical treatment and rehabilitation of patients with limb loss. Moscow, “Geotar-Media”, 2015. p. 11.

