
Manuscript accepted on :December 20, 2016
Published online on: --
Plagiarism Check: Yes
Heidar Ali Esmaili1, Bahareh Mehramuz1, 2, Parham Maroufi3, Ateyeh Ghasemi4 and Tala Pourlak5, 6*
1Department of Pathology, Alzahra Hospital, Tabriz University of Medical Sciences, Tabriz, Iran.
2Hematology and Oncology Research Center, Tabriz University of Medical Sciences, Tabriz, Iran.
3Department of Orthopedic, Tabriz University of Medical Sciences, Tabriz, Iran.
4Drug Applied Research Center, Tabriz University of Medical Sciences, Tabriz, Iran.
5Department of Pathology, Imam Reza Hospital, Tabriz University of Medical Sciences, Tabriz, Iran.
6Connective Tissue Diseases Research Center, Tabriz University of Medical Sciences, Tabriz, Iran.
Corresponding Author E-mail: dr.pourlaktala@yahoo.com
DOI : https://dx.doi.org/10.13005/bpj/1120
Abstract
One of the causes of acute abdomen is acute pancreatitis. Usually when there is an increase in pancreatic enzymes including amylase and lipase levels three times higher than normal, the diagnosis of pancreatitis is made. Our study focused on the diagnostic value of amylase and lipase in the diagnosis of acute pancreatitis with sensitivity, specificity, positive predictive value and negative predictive value. This study is a descriptive-analytical study examined 458 patients with acute abdomen who were referred to emergency department of Imam Reza Hospital of Tabriz. Information compiled a checklist and analysis software has been SPSS 15. The results show that among 458 studied patients, 189 (41.3%) was men and 269 patients (58.7%) were women. 88 (19.2%) patients had diagnosis of acute pancreatitis. In patients with acute pancreatitis, amylase average was 397.17 IU/L. Among patients with acute pancreatitis, blood amylase of 22.7 % were ≤ 110 IU/L, 35/2% were in the 330-110 IU/L and 42% were ≥330 IU/L. Diagnostic accuracy of amylase for cutoff 110 IU/L was as follows: sensitivity= 79.2%, negative predictive value (NPV)= 92% (suitable), positive predictive value (PPV) = 43%, specificity= 69% (not suitable and could not help to diagnose). Diagnosis accuracy of amylase for cutoff in 330 IU/L was as follows: specificity= 92%, NPV= 84% (suitable for diagnosis), sensitivity= 42%, PPV= 61%, (not suitable and could not help to diagnose). Study shows average lipase level in patients with acute pancreatitis was 399 IU/L. Among 19.3% of patients with acute pancreatitis, the blood lipase was ≤80, 22.7 % were in 240-280 IU/L, and 58% was upper than 240 IU/L. Diagnostic value of lipase, for cut off 80 IU/L was as follows: sensitivity=80%, NPV= 92% (suitable for diagnosis), but specificity= 69% and PPV= 44% which were not suitable for diagnosis. For cut off In 240 IU/L specificity= 88%, NPV= 87% (suitable for diagnosis) but sensitivity= 57% and PPV= 58% not suitable and could not help to diagnose. Our study showed that levels of lipase and amylase enzymes are helpful for diagnosis of acute pancreatitis. Different diagnostic thresholds for each enzyme assay have different sensitivity and specificity. Therefore, that by increasing the level of diagnostic threshold, specificity of tests increases but there sensitivity decrease. In our study, the diagnostic threshold of the negative predictive value was acceptable but the positive predictive value was unacceptable.
Keywords
Amylase; Lipase; Acute Pancreatitis
Download this article as:| Copy the following to cite this article: Esmaili H. A, Mehramuz B, Maroufi P, Ghasemi A, Pourlak T. Diagnostic Value of Amylase and Lipase in Diagnosis of Acute Pancreatitis. Biomed Pharmacol J 2017;10(1). |
| Copy the following to cite this URL: Esmaili H. A, Mehramuz B, Maroufi P, Ghasemi A, Pourlak T. Diagnostic Value of Amylase and Lipase in Diagnosis of Acute Pancreatitis. Biomed Pharmacol J 2017;10(1). Available from: http://biomedpharmajournal.org/?p=13503 |
Introduction
In acute pancreatitis, blood amylase increased. Sometimes up to 6-4 times the highest normal level rises (1). Amylase levels also in other diseases, such as pancreatic duct obstruction, pancreatic cancer and biliary problems specifically rise. Several types are called amylase isoenzyme. Different tissue make various types which normally seen in the blood and urine although law levels (2). When pancreatic tissue damage (eg. pancreatitis) or pancreatic duct is blocked, serum amylase levels increased. It should be noted that the normal range for amylase concentration is 15-110 IU/L (2).
In acute pancreatitis, lipase levels are often very high; 10.5 times the normal level can be increased (3). The average increase in lipase can be seen in other conditions such as kidney disease, inflammation of the salivary gland, intestinal obstruction or ulcer but usually does not apply to these measured levels of lipase (4). It should be noted that the normal range lipase concentrations is 10-80IU / L(5).
This study aimed to determine the diagnostic value of amylase and lipase in the diagnosis of acute pancreatitis with Sensitivity, Specificity, PPV and NPV.
Methods and Materials
The samples were selected from 400 patients referred to Imam Reza hospital because of acute abdominal pain and suspected acute pancreatitis. This study was conducted over 24 months and was done in Imam Reza Hospital emergency department.
Patients amylase and lipase were done by conventional biochemical tests (6-8), patients data were collected from Laboratory data bank, and information were noted in checklists.
Through study of patients, folders and regarding to acute pancreatitis diagnostic criteria’s, patients were divided into two groups: 1) acute pancreatitis 2) individuals and patients without acute pancreatitis.
Statistical analyses were done according to Table 1 formula for calculating TP, FP, TN and FN. It should be noted that the determination of the above mentioned statistics was carried out in two separate Cutoffs (9).
Results
The results showed that among the 458 studied patients, 189 (41.3%) were men and 269 (58.7 %) were women. The average age of our studied patients was 58 years; the minimum age was two and maximum were 102 years old.
The frequency of acute pancreatitis in our study, 88 patients (19.2%) had acute pancreatitis was
Investigation amylase levels showed that average total factor 209.7 patients varied from a minimum of 9.5 to a maximum of 2100. In patients with acute pancreatitis amylase average of at least 9.5 up to 1835 was 397.17 was variable.
Regarding results of blood amylase in 59.8 % were less than normal number (110), and also 25.1% and 1.15 were nearly by 110 and 15.1% were more than 330. Throughout the patients with acute pancreatitis, blood amylase 22.7 percent were less than the 110, and 35.2% about 110 and 42 percent were more than 330.
Table 1: statistical indicators were calculated according to a specificity and sensitivity formula.
| Normal | Acute pancreatitis |
: patients Test |
| FP**$ | TP*# | Positive |
| TN**$ | FN*# | Negative |
* Sensitivity = TP/(TP+FN) **Specificity = TN/(TN+FP)
#PPV = TP/(TP+FP) $NPV = TN/(TN+FN)
The low positive predictive value indicates that the results do not match the clinical results and the area under the ROC curve with 0.08 cannot be titled as diagnostic value. However, in determined cutoff point, which in this study is 330, specifity 0.923, negative predictive value. 0.84 were appropriate but sensitivity 0.42 and positive predictive value 0.61 does not mean as a predictive paramete or accurate.
The low sensitivity, low power indicator is in the correct diagnosis of the patient. In addition, low positive predictive value indicates that the results are not consistent with clinical outcomes.
Investigation lipase values show that average total factor 192.3 patients can vary from a minimum of 8 to a maximum of 2850. In patients with acute pancreatitis, lipase levels average were about 399, which varies from a minimum of 16 to a maximum of 1764. Regarding results blood lipase levels in 59.4 % were less than normal number (80), and 19.7% were nearly by 80-240 and 21% were more than 240. Throughout the patients with acute pancreatitis, blood lipase 19.3 percent were less than the 80, and 22.7%, about 80-240 and 58 percent were more than 240.
The results of our study showed that the diagnostic value lipase shows Cutoff point = 80 sensitivity and negative predictive value with the value 0.807 and 0.92 are appropriate to evaluate the diagnostic value. However, specifity 0.69 and positive predictive value 0.44, has no diagnostic value. The low positive predictive value indicates that the results are not consistent with clinical outcomes. The area under the ROC curve with the 0.83 ability to show proper diagnosis.
In addition, our study showed that the diagnostic value lipase shows Cutoff point = 240 sensitivity and positive predictive value 0.57 and 0.58 are not appropriate to evaluate the diagnostic value. However, specifity 0.88 and negative predictive value 0.87, has diagnostic value. The low sensitivity, low power indicator is in the correct diagnosis of the patient. Moreover, low positive predictive value indicates that the results are not consistent with clinical outcomes. Area under the curve is equal to the ROC 0.471 that cannot show a proper diagnosis.
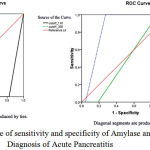 |
Figure 1: ROC curve of sensitivity and specificity of Amylase and Lipase in Diagnosis of Acute Pancreatitis
|
Discussion
The present study noted that lipase enzyme is selective for the diagnosis of acute pancreatitis because its specific for pancreas and according to selective detection threshold sensitivity and specificity is different.
Increased levels of amylase enzyme activity at least 3times in consecutive tests, should be more than maximum amount of its normal to be able to distinguish acute pancreatitis (10-11).
Sensitivity and specificity of amylase as a diagnostic test for acute pancreatitis depends on the threshold set for it are (in our study was 110 and 330). By increasing the threshold (cut off) to 1000 IU / L (more than three times the upper limit of normal), specificity was 95% but its sensitivity is reduced to 61% (12-14).
In our study, both by increasing the diagnostic threshold of 110 UI / L to 330IU / L diagnostic sensitivity decreased (from 79% to 42% decreased) but instead increased diagnostic specificity (from 69% to 92% increase). In both the threshold value and negative predictive value, positive predictive value was appropriate but did not have a proper diagnosis.
Serum lipase compared with serum amylase increased for longer remains and in patients with late symptoms is good sensitivity. As well as amylase, lipase, specific for the diagnosis of pancreatitis is not specific (15-17).
Lipase has better accuracy than amylase (18). In one study, the diagnostic threshold lipase 600 IU / L at 95% specificity and sensitivity between 55-100% and by increasing the diagnostic threshold (600 IU / L <) increase the specificity and sensitivity is reduced.
In our study, together with the increase in the threshold of detection of 80 IU / L to 240IU / L specificity of 69% to 88% increased from 80% to 56%. Instead, test sensitivity was reduced. In both diagnostic thresholds good negative predictive value and positive predictive value was inappropriate and diagnostic value.
Treacy and colleagues conducted a study to evaluate 1,598 patients with acute abdomen who were 44 cases of acute pancreatitis and the average age of the participants was also 6/49 years (19). In addition, the diagnostic threshold (3 times more than normal) 900IU / l for lipase and 330IU / l for amylase had intended. In this study, the diagnostic threshold will increase to five times the normal range (20-21).
Sensitivity and specificity were respectively 99% and 39%. While the diagnostic threshold to 3 times normal range did not change, but the specificity decreased sensitivity increased to 50%. In case lipase 5 times higher than the normal range in both the detection threshold sensitivity 98% and specificity of 57% was obtained and when the threshold to 3 times higher than the normal range dropped 97% specificity and 64% sensitivity (22), respectively. In the range of 99-98% negative predictive value of both tests regardless of the diagnostic threshold for amylase and positive predictive value of 50% at 5 times the normal diagnostic threshold and 51% in diagnostic Sanh was 3 times normal. The positive predictive value of 50% for lipase at 5 times the normal diagnostic Sanh and 41% in diagnostic threshold was 3 times normal (23). In this study, the diagnostic accuracy for amylase (area under the curve ROC) on the eve of the eve of the 330 110 8% and 94%, which shows that we are on the verge 330 more accuracy and are more reliable. In addition to lipase close to 80 times the diagnostic accuracy of 84% and 47% respectively in the 240 threshold, this result indicates that the diagnostic accuracy for lipase in our study on the verge of 80IU / L more (24) .
Steven and colleagues reported in a study in the diagnostic threshold of 240 U / L for amylase and 800U / l for lipase, the sensitivity, specificity and diagnostic accuracy for amylase were respectively 69%, 79%, 76% and 80% for lipase, 84% and 82% (25).
In our study, the diagnostic accuracy for amylase was at threshold 330 was and lipase almost the same is also on the verge of 80 which indicates that we need to high blood levels to increase the diagnostic accuracy for amylase But for lipase do not require a high level of enzymes to detect and in case of clinical symptoms of pancreatitis can be diagnosed with a slight increase lipase levels raised. Steven and Associates study also was among the 508 patients, 180 (35%) experienced an episode of acute pancreatitis were 36% male and 64% were female. In our study, 88 patients (19%) had acute pancreatitis which were 42% male and 58% were women, almost like the high incidence of acute pancreatitis in women, but the reason for this was not found (26). In another study that was conducted to assess the level of amylase and lipase in acute pancreatitis (threshold to 240 for amylase and lipase 600), the average level of amylase was 353u / l and the average level of lipase was 2745u / l. In this study actual positive, false negative, actual negative and false positive for amylase and lipase respectively were 77, 29, 627, -124 and 104, 2, 723, 28. These amounts are almost the same (in terms of ratio) our study is at threshold of 110 for amylase and 80 for lipase. In our study Cut Off = 110 for amylase, and negative predictive value (NPV) is the appropriate with 0.920 but positive predictive value (PPV) of 0.432, could not have a proper diagnosis = 330 Cutoff negative predictive value of 0.82 is good, but the positive predictive value of 0.61, cannot be accurate. In this case, the low positive predictive value in both the threshold suggests that the results are not consistent with clinical outcomes. Also, 80 = Cut off for lipase negative predictive value of the diagnostic value is 0.92 appropriate to investigate. However, the positive predictive value of 0.44, not have diagnostic value. In Cutoff= 240 the negative predictive value with amount of 0.87 is appropriate to evaluate the diagnostic value. However, the positive predictive value of 0.58 does not have diagnostic value. In addition, low positive predictive value in both the threshold indicates that the results do not match with clinical results. In a study by James and colleagues of 110 threshold for amylase and 240 for lipase were considered, 0.38 and 0.78 respectively were positive predictive value and negative predictive value 0.95 and 0.99 (27). As we see the negative predictive value was similar in both study nearly threshold the same. This shows that the tests are successful in anticipation people, who do not suffer, but in our study, the positive predictive value for both enzymes is low and these tests are not predictive ability of full cases and should be matched with clinical symptoms.
Conclusion
Our study showed that levels of lipase and amylase enzymes are helpful for diagnosis of acute pancreatitis and compared to different thresholds for each enzyme assay sensitivity and specificity can be achieved differently So that by increasing the threshold on the diagnostic specificity and sensitivity of the test increases will be reduced. In our study, the different diagnostic thresholds of each enzyme were acceptable predictive value. However, the positive predictive value was unacceptable and did not match with clinical results. Therefore, more research needs to be done to investigate the matter.
Acknowledgment
The present study was supported by Tabriz University of Medical Sciences. We thank all staff of Imam Reza Hospital Laboratory and Alzahra Hospital Laboratory for their cooperation.
Conflict of Interest
None to declare
References
- JWY Chang, CH Chung (2011). Diagnosing acute pancreatitis: amylase or lipase? Hong Kong Journal of emergency medicine, 18: 20-25.
- James P. Corsetti, Christopher Cox, Thadeus J. Schlz, and Dean A. Arvan (1993). Combined Serum Amylase and Lipase Deteriminations for Diagnosis of Suspected. CLIN CHEM. 39/12, 2495-2499.
- Ahmed Z. Al-Bahrani, Basil J. Ammori (2005). Clinical laboratory assessment of acute pancreatitis. Clinica Chimica Acta, 362: 26-4.
- Peter A. Banks, et al (2006). Practice Guidelines in Acute Pancreatitis. Am J Gastroenterol, 101: 2379-2400.
- Cappell MS (2008). Acute pancreatitis: etiology, clinical presentation, diagnosis, and therapy. Med Clin North Am, 92(4), 889-923.
- AbouRjaili G, Shtaynberg N, Wetz R, Costantino T, Abela GS (2010). Current concepts in triglyceride metabolism, pathophysiology, and treatment. Metabolism. J Clin Gastroenterol, 1210-20.
- Asgharzadeh M, Kafil HS, Ebrahimzadeh ME, Bohlouli A (2007). Mannose-binding lectin gene and promoter polymorphism and susceptibility to renal dysfunction in systemic lupus erythematosus. J Biol Sci 7 (5), 801-805
- Havel RJ (1969). Pathogenesis, differentiation and management of hypertriglyceridemia. Adv Intern Med, 15:117-54.
- Hokanson JE, Austin MA (1996). Plasma triglyceride level is a risk factor for cardiovascular disease independent of high-density lipoprotein cholesterol level: a meta-analysis of population-based prospective studies. J Cardiovasc Risk, 3(2):213-9.
- Ewald N, Kloer HU (2009). Severe hypertriglyceridemia: an indication for apheresis? Atheroscler Suppl. 29;10(5):49-52.
- Yeh JH, Chen JH, Chiu HC (2003). Plasmapheresis for hyperlipidemic pancreatitis. J Clin Apher, 18(4):181-5.
- Charles Brunicardi F, Michael E (2010). DeBakey Department of Surgery, Baylor College of Medicine, Houston, schwartz s principal of surgery, 9: 540-561.
- Cole RP (2009). Heparin treatment for severe hypertriglyceridemia in diabetic ketoacidosis. Arch Intern Med, 169:1439-41.
- Bensadoun A(1991). Lipoprotein lipase. Annu Rev Nutr,217-37.
- Matull WR, Pereira SP, O’Donohue JW (2006). Biochemical markers of acute pancreatitis. J Clin Pathol, 59(4):340-4.
- Asgharzadeh M, Kafil HS, Khakpour M (2008). Comparison of mycobacterial interspersed repetitive unit-variable number tandem repeat and IS6110-RFLP methods in identifying epidemiological links in patients with tuberculosis in Northwest of Iran. Annal Microbiol, 58(2): 333-9.
- HUMES S, SMITH P, WRIGHT W, LOBO M (2009). The role of routine assays of serum amylase and lipase for the diagnosis of acute abdominal pain. Ann R Coll Surg Engl, 91: 381–384.
- Gumaste VV, Roditis N, Mehta D, Dave PB (1993). Serum lipase levels in nonpancreatic abdominal pain versus acute pancreatitis, Am J Gastroenterol, 88: 2051–5.
- Treacy J, Williams A, Bais R, Willson K, Worthley C, Reece J et al (2001). Evaluation of amylase and lipase in the diagnosis of acute pancreatitis. Aust NZ J Surg 71: 577–82.
- Orebaugh SL (1994). Normal amylase levels in the presentation of acute pancreatitis. Am J Emerg Med 12: 21–4.
- Corsetti JP, Cox C, Schulz TJ, Arvan DA (1993). Combined serum amylase and lipase determinations for diagnosis of suspected acute pancreatitis. Clin Chem 39: 2495–9.
- Yadav D, Agarwal N, Pitchumoni CS (2002). A critical evaluation of laboratory tests in acute pancreatitis. Am J Gastroenterol 97:1309–18.
- Werner J, Feuerbach S, Uhl W, et al (2005). Management of acute pancreatitis. surgery to interventional intensive care. Gut 54:426–36.
- W R Matull, S P Pereira, J W O’Donohue (2002). Biochemical markers of acute pancreatitis. J Clin Pathol 59:340–344.
- Steven C. Kazmierczak. Paul G. Catrou,’ and Frederick Van Lente (1993). Diagnostic Accuracy of Pancreatic Enzymes Evaluated by Use of Multivariate Data Analysis. CUNICAL CHEMISTRY, Vol. 39, No. 9, 1960-1965.
- Courtois P, Gnat D, Wenders G, Vertongen F, Franckson JRM (1986). Interet du dosage simultane de l’alpha-amylase et de in lipase pancreatique pour le diagnostic des as aigus de pancreatite. Rev Med Brux 7:527-32.
- James P. Corsetti, Christopher Cox, Thadeus J. Schulz, and Dean A (1993). Aryan’ Combined Serum Amylase and Lipase Determinations for Diagnosis of Suspected Acute Pancreatitis. Clin Chem 39: 2495-2499.

